

A Dark Horse Variant Is the Holiday Winner
Collateral damage in the war on Polio

Back on October 26th I first mentioned the COVID variant JN.1. Only a small number of sequences around the world had been reported by then, but there had been enough in France for some astute modelers to predict a sizable growth advantage over the other most common variants. Since then JN.1 has come on very quickly, and as of last week it was the second most common COVID variant in the US, and destined to become number one within another week. You may recall that JN.1 is almost identical to BA.2.86, the variant dubbed Pirola, with only a single spike mutation providing the enhanced infectivity compared to its parent. The WHO declared JN.1 a variant of interest (VOI) last week, while suggesting that it did not pose any more significant public health risk than current variants. This is a major evolutionary pivot for COVID away the XBB family of mutants which have dominated for over a year now, to a member of the BA.2 family with a large novel combination of mutations, plus the L455R spike mutation providing enhanced immune escape. Whenever a new, rapidly expanding COVID variant appears during a period of escalating disease, we are informed that epidemiologists have no idea whether this new virus is driving the increase in cases. That is true, there are so many variables at work: social behavior, density of indoor congregation, reflecting weather and holidays (Taylor Swift concerts), the community immunity landscape, reflecting vaccination and timing of previous waves of specific variants. It is tempting however to assume that a variant like JN.1, which has significantly enhanced immune escape, and is so rapidly outcompeting the other previously dominant species, just might be playing a major role in the current increase in cases.
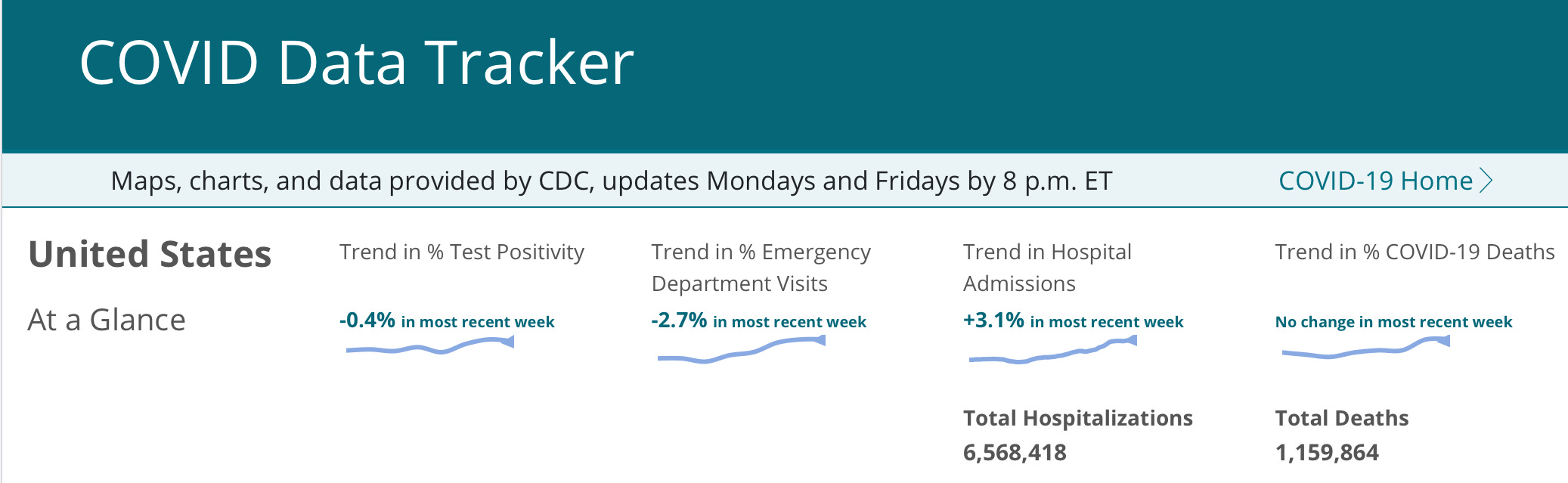
Of course we don’t actually have any accurate handle on case numbers anymore. We can look at hospitalizations as some surrogate, and they have continued their upward trend to over 23,000 in the previous week. How about deaths? That should be incredibly easy to spot, however the CDC decision quite a while back to express COVID deaths as a percentage of total deaths rather than a simple number obfuscates that a bit. COVID deaths are plateaued at about 3% nationally. If you assume a current death rate for hospitalized people of 5%, then this would be about 1200/week. Another, perhaps more accurate approach, is to use the total mortality from prior years. If we use as a baseline pre-pandemic 2019, then the current calculated COVID deaths would be 1647/week. Realistically, we have a lot more people dying from fentanyl and a number of other issues now than 2019, plus approximately 8.5 million illegal migrants over the last 3 years, so lets use the total deaths in 2022 as a guide, and that calculates to 1888 COVID deaths/week, or a 9/11 death toll every 2 weeks, just like clockwork. Collective amnesia and ignoring unpleasant realities may be a useful human coping mechanism for psychic pampering and societal stability—but if you are in a high risk group for severe COVID disease then an updated booster is a better bet for physical health, than the head in the sand approach. This past week the CDC issued an urgent plea for healthcare providers to increase their engagement with the public to try and increase the dismal vaccination numbers. As of the latest data available only 17% of adults, and 33.3% of folks over 65, had taken the new fall COVID booster. The over 65 yo. group of course represents the vast majority of COVID deaths. The Influenza vaccination level is also running behind recent historic norms at 40% of the eligible population. Surprisingly the rate of Influenza vaccination among health care workers is currently about 3% lower than historic norms as well—is it vaccine fatigue?

Next I want to revisit an issue which I have been very concerned about for several years, and have discussed previously in this news letter, the problem of circulating vaccine derived Polio virus. Africa was declared Polio free in 2020 after a number of years with no cases of Wild Type (WT or natural Polio). But that didn’t mean there were no cases of paralytic disease caused by a Polio virus. The attenuated virus used in the production of the oral polio vaccine has mutated in recipients over time, and has been circulating around Africa and other areas of the world, causing the paralysis of hundreds of children every year. You may recall that we had a case of vaccine related Polio in New York this year. The unlucky individual had not received the vaccine himself, but had been infected by someone who acquired the mutated vaccine derived virus in another country and was excreting it. Scientists and Public Health officials, particularly the WHO, knew of this risk, and of the community circulation of the mutated virus, which is just as dangerous as natural WT Polio, but have continued mass immunization campaigns with this oral vaccine. To quote Paul Offit, one of the most senior and respected vaccine scientists in the country, “"We were seduced by the fact that it was cheap. It caused contact immunity. It was easy to give," Offit says. "And so we thought, 'We can eliminate this disease in the world.” The Global Polio Eradication program was initiated in 1986 with a goal of Polio eradication by 2000, but a quarter century after that date, it appears they were wrong, and in my opinion the entire approach needs to be re-thought.
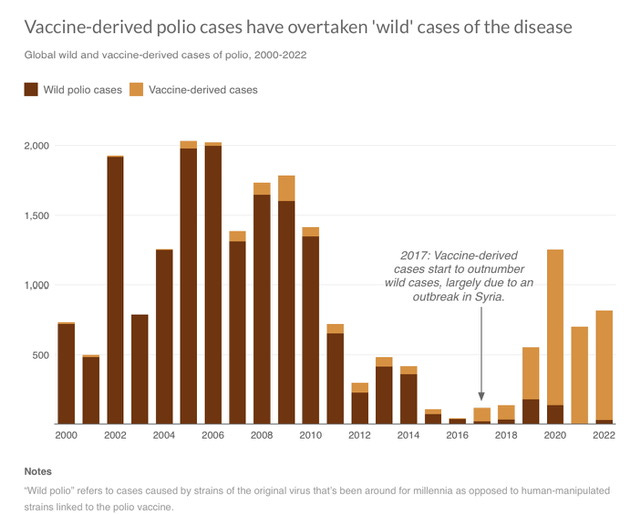
A handful of natural WT Polio cases occur in two countries every year, Afghanistan and Pakistan. Natural Polio has been eliminated in many severely impoverished and remote locations around the world, but in Afghanistan and Pakistan the public health authorities have to contend with those obstacles as well as fanatic Islamists who have a penchant for murdering vaccine distributors and cowering the villagers into shunning vaccination. In Malawi in 2022 a single case of WT Polio surfaced, which was genetically determined to be identical with the WT virus in Pakistan, in other words, it was imported. The response of the WHO was to begin multiple rounds of millions of oral Polio vaccinations for the entire country, and two adjacent countries where several other cases of the imported Polio were found. Even if you vaccinate every child in these countries, it is established fact that many poorly nourished kids in tropical countries with a variety of other infections do not respond to the current oral vaccine at a level sufficient to prevent infection. As Paul Offit further observed, “… we have unleashed a dragon, and that is the oral Polio vaccine.” If you think pouring gasoline on a kitchen fire is a smart approach, perhaps there’s an opening for you at the WHO. Below is a picture of how well that strategy has been working. You will see just how long vaccine derived mutated Polio virus has been freely circulating in the world, and how cases of paralytic disease caused by it now vastly eclipses the handful of WT cases in the world. So far this year the Democratic Republic of Congo has recorded 90 children paralyzed by vaccine strain Type 1 and 109 paralyzed by vaccine strain Type 2, with zero cased of WT Polio. In Nigeria it’s 55 and counting from vaccine Type 2. Just to be clear, the vaccine we use in the US is the inactivated injectable vaccine—it can not ever cause this problem and further will completely protect you from infection.
The winter respiratory virus season is ramping up now as expected, not just COVID but the old standbys of Influenza, RSV, parainfluenza and the typical cold viruses. Very few of us seem inclined to wear masks anymore, and vaccine fatigue seems to be a real phenomena—so what does the future look like; are we just consigned to endless bouts of respiratory disease? I think we have learned some important lessons during the Pandemic that fall into the category of potentially very helpful, and are totally passive, requiring no behavioral adjustments or controversy. First we should be adopting high grade air filtration, and incorporating this capacity into all new construction, along with the ability to adjust HVAC systems to variably increase fresh air intake on demand. UV light is a very effective germicide, but its use has been limited by human skin and ocular toxicity. Standard UV light has been used extensively in hospitals to rapidly decontaminate patient rooms and operating rooms, but without humans present during use. The wavelengths called UV-C or Far UV light from 230-200nm have been shown to be quite safe in animal exposure. These very energetic wavelengths of UV are totally absorbed in the layer of skin called the stratum corneum, which is composed of dead, non-replicating cells. Recent experiments have demonstrated that easily tolerated energy levels in this spectrum have the ability to very significantly decontaminate an indoor air space with the constant addition of SARS2 virus. This replicates an indoor environment where infected people are continuously adding virus to the air. (We all knew that wearing a mask for the minute it took to walk to your table in a restaurant where you would be unmasked for over an hour was total nonsense and compliance theater). Evidence would have to accrue that UV-C is indeed safe for direct human exposure, but I can easily envision air circulation patterns which would direct the air stream to the ceiling where it would be bathed in UV-C shielded from direct exposure to room occupants.
The editorial department is reminding me that I still have Christmas shopping to do and they are anxious to be heard before the end of 2023. They have investigated, and are prepared to fact check some internet disinformation.
A rumor is circulating that the US government has taken note of the vast sums to be made in the entertainment space, and in order to reduce the now 34 trillion dollar debt have started a film production unit. While the White House production of the classic, “The Nut Cracker” could legitimately be a first effort—there is absolutely no truth to the conspiracy theory that the video of two young cowboys bare-backin’it in the Senate is a short trailer for a feature DC sex romp starting Donald Trump and President Biden. Our investigators have definitively determined that any plans for this were tabled after Trump refused the casting team’s directive to hit the gym and Ozempic, and Biden couldn’t remember his lines.
It is pure conspiracy theory that the Harvard Board will find a way to rid themselves of President Claudine Gay. They note that she has already issued an OOPS DO OVER for her obviously pre-prepared statement to Congress that calls for genocide against Jews must be viewed in “context”; and that her lighting the campus menorah with a Tiki-Torch, was reasonable, since it wasn’t one of those racist Right-Wing Tikis. Beyond that the University has decided that plagiarism is totally cool, even a little edgy, if you meet certain DEI criteria.
Kamala Harris was awarded the prestigious Cicero Prize for best rhetoric by a US politician for whom English is a second language. Fact checked and totally false.
Thanks for your attention to this short holiday week update. The sound you hear on the roof is not reindeer hooves but the sound of readers like you hitting the like and share buttons. The very best to everyone from the staff of “Clear and Present Thinking”. Comments conforming to strict DEI standards and devoid of micro-aggressions are welcome.
Merry Christmas and see you in the New Year !
I maybe coming out in Jan
I will let you know
Renee
The polio thing is soooo scary! I remember standing in line with my dad at the firestation while we waited for the sugar cube vaccine...I'm now feeling the pain of that worthless POS!
Keep up your good work:)