

BQ.1.1 Variant, Your Uninvited Thanksgiving Guest

First up today is the good news, because we are certainly due for some. In recent weeks I’ve been highlighting the severe stress on the US Pediatric Health system due to the wave of respiratory virus illness, particularly the unusually high RSV activity. Unlike COVID right now, this virus is hospitalizing large numbers of very young children around the country. This week Pfizer released top line data on its phase 3 RSV vaccine for pregnant women, and the results are excellent. Let’s just take a moment to review some of the problems inherent in trying to protect children from RSV. The group at the very highest risk of severe disease are newborns in the first couple of months of life. That is also the group with immature immune systems which often fail to respond adequately to vaccines, or infections for that matter. Even if they did respond well, the greatest need for protection is immediately after birth; and as we all know it can take more than one dose of vaccine, (5 and counting?) to obtain good protection from respiratory viruses. The solution is to vaccinate the mother during pregnancy so she shares her mature antibody response with the infant. This new formulation circumvents a serious problem encountered with earlier attempts at making an inactivated virus RSV vaccine, referred to as ADE or antibody dependent enhancement. This candidate vaccine will provide no immediate relief to the current surge situation, and it will face all the usual regulatory scrutiny before eventual approval. Here are the results from Pfizer’s press release.
The pre-planned, interim efficacy analysis conducted by an external and independent Data Monitoring Committee (DMC) met the success criterion for one of two primary endpoints. The observed efficacy for severe medically attended lower respiratory tract illness (severe MA-LRTI) was 81.8% (CI: 40.6%, 96.3%) through the first 90 days of life. Substantial efficacy of 69.4% (CI: 44.3%, 84.1%) was demonstrated for infants over the six-month follow-up period.
82% vaccine efficacy in preventing RSV severe enough to require medical intervention during the first 3 months of life is outstanding. The fact that efficacy is declining over the next 3 months is expected since the maternal antibodies are fading away, and is of less importance since the vast majority of severe RSV outcomes occur in the first couple of months. Although usually thought of as a pediatric disease, RSV also causes substantial morbidity and mortality in the elderly and immune compromised; with the CDC reporting 177,000 hospitalizations/year and 14,000 deaths in people over 65 years old. The further good news is that in August Pfizer released results of its Phase 3 trial of their RSV vaccine candidate in adults over 60, and showed an 85.7% efficacy in preventing severe lower respiratory tract illness. This is a traditional, bivalent protein vaccine, so any consideration of mRNA hanky-panky during pregnancy is mute.
I have exhausted the good news so let’s move on to “Post Truth Era” reality of COVID. Here are the most recent graphs of COVID cases, hospitalizations and deaths.

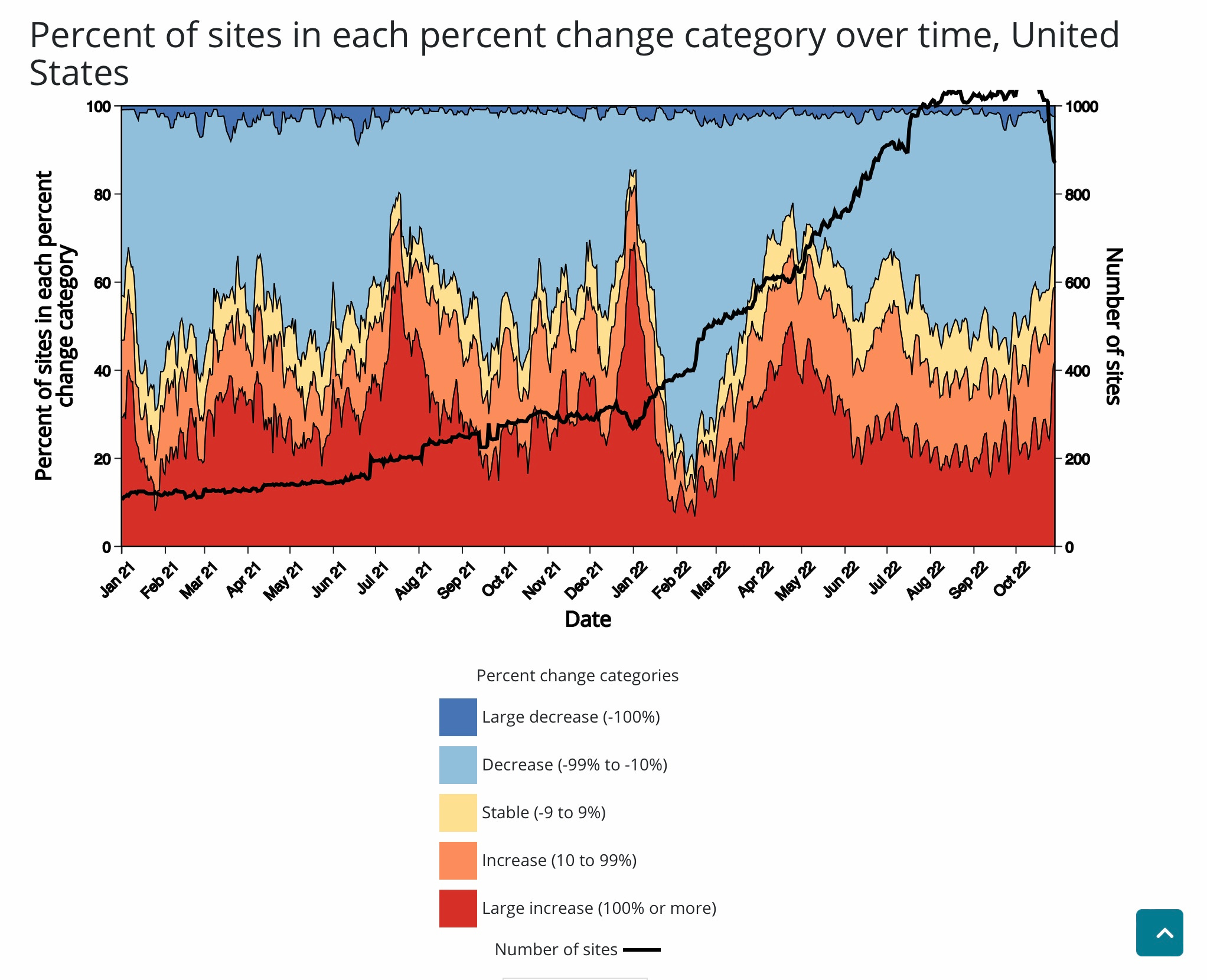
The Pandemic which is “over” is continuing to claim, at a pretty steady pace, a 9/11 style US death toll every week. 21,000 people are hospitalized on any given day. Uptake of the new bivalent boosters remains quite low and is not accelerating. If this is the “new normal” then I suppose people are quite justified in trying to ignore it—“have to move on sometime” I suppose. The question is, has Mr. COVID decided this is the new status quo; after all the virus has an important contribution to the discussion. The declining curve of new cases above looks pretty good, but it is essentially meaningless. The disconnect between the number of reported cases and the actual prevalence of COVID disease in the community has rapidly widened as testing and self reporting of positive results has cratered. The CDC map of community disease prevalence and new daily cases is a sham; I know it, you know it, and the CDC knows it—but many people do not. What does waste water surveillance tell us? The CDC graph below can be a bit tricky to interpret, but it shows that in the last 4 weeks the majority of waste water systems which are being tested around the country are showing a significant increase in the virus. The red and orange area increasing from a trough in late September, and the blue area decreasing is the key. As a result of this new reality, Public Health Departments around the country are moving away from tracking positive tests, and concentrating on metrics like hospitalizations and waste water COVID levels.
The newest COVID variants are expanding right on cue, and as I predicted about a month ago, they now represent more than 50% of the circulating virus. The most likely winners in the race here appear to be BQ.1, BQ.1.1 and BF.7. They are doubling as a percentage of viral sequences about every 10 days. We know from laboratory studies that they are more immune evasive with respect to panels of monoclonal antibodies than preceding Omicron’s, including BA.5. In any event it’s a good bet that BA.5, which our shiny new bivalent boosters were designed to target, will be history or at least a small minority of the circulating virus within a few weeks. So far the published data suggests that against BA.5 the new boosters were a wash (or slightly better) than the original vaccine boosters. That may not matter much at all in a few weeks. How will they perform against the new swarm of B’s, which appear to be increasing the reinfection rate? That’s anyone’s guess right now, we don’t have any data on that yet. On June 5th I opined that BA.5 would be the uninvited guest at your 4th of July celebration, now it will be time for BQ.1 at the turkey feast. As of this moment there is no indication of increased disease severity or hospitalizations, just an increased ability to infect folks with prior vaccine, booster and natural immunity. The wave of diagnosed XBB variant in 94% vaccinated Singapore is beginning to subside, without having caused much of an increase in hospitalizations. It’s too early to draw firm conclusions given the characteristic 2 week delay in hospitalization increases; and also, it looks like we will be dealing with BQ.1 here and not XBB. The situation in France also looks promising at the moment. Their 7th wave started earlier than here, and peaked quickly, with a only a small increase in hospitalizations which are now trending down. The French experience is likely more applicable to what we may expect in the US, since BQ.1 is now their dominant variant du jour. It is quite possible that our accumulated T cell immunity, which is broader and more adept at intercepting novel variants than our neutralizing antibodies, is finally gaining the upper hand, and preventing the vast number of infections from becoming severe. Keep in mind that if the winter wave accelerates, with new variants that are more easily sidestepping the temporary increase in protection from boosters: N95 masks, increased indoor ventilation and avoiding crowded spaces—those old low tech annoying mitigations—will still be effective in reducing risk no matter what variant shows up.

In the last section today are several rapid fire items of information and opinion. I was disappointed to read that a handful of Universities, including Harvard, Yale and Fordham, will be mandating the new bivalent boosters for their students. Given everything we know right now, to say this is illogical, and a serious infringement on individuals’ rights of healthcare choice would be an understatement. If you are an older professor, or an immunocompromised student, or you just want another shot, by all means do so. Don’t imagine though that forcing your fellow student to take ANOTHER booster will prevent them from either catching the disease or spreading it. Healthy college age students by this time in the pandemic have sufficient immunity, from multiple prior vaccinations and extremely high rates of prior infection, to protect them from severe disease. It is old, infirm and immunocompromised people who are landing in the hospital and dying today, not healthy 20 year olds.
If you ever felt disheartened after catching COVID when you thought you were being very careful, the following paper from the December 2022 issue of Emerging Infectious Diseases will give you a perspective on just how incredibly transmissible the Omicron variant is. This is a study out of Taiwan, where strict quarantine of incoming travelers was a major part of their strategy to avoid the virus. Fifteen clusters of infection without obvious contact between the quarantined people were reported. In this paper the investigators show how the virus almost certainly traveled by aerosol dispersion through walls and between floors to non-adjacent rooms causing infection. The CDC and the WHO were dead wrong for half a year AFTER the evidence of aerosol transmission was clear, both in the environmental science and engineering literature, and from mass spread events like the Washington state choir outbreak. Probable Aerosol Transmission of SARS-CoV-2 through Floors and Walls of Quarantine Hotel, Taiwan, 2021
Finally there is a paper from the UK on the transmission dynamics of Monkey Pox. The short version is that they are demonstrating (both through epidemiological models and individual contact tracing chains of infection) that there is very significant spread of the virus during the pre-symptomatic period. Yes, the MPX world wide epidemic is subsiding to great relief, but this new finding ups the ante that it may turn out to be impossible to eradicate the virus from the new regions of the world it has expanded into. That’s a shame, one more despicable little bundle of DNA and protein to spread misery and death—COVID, Vladimir Putin and his troglodyte Kremlin cronies should have been quite enough.
Transmission dynamics of monkeypox in the United Kingdom: contact tracing study | The BMJ https://www.bmj.com/content/379/bmj-2022-073153
Thanks for catching up with the infectious disease news. I’m grateful to everyone who has shared Clear and Present Thinking with their friends and colleagues, and I will ask you to continue spreading the word. Remember my dopamine receptors with the like button if you found the update valuable. In the comments you can indicate if you would prefer more in-depth analysis of international Cricket scores, or a list of my favorite K-Pop bands.