

Cancer in the News

There being little of immediate interest regarding COVID in the scientific literature, I want to address the story dominating the news cycle this week, which is President Biden’s apparently just discovered stage 4 prostate cancer with bone metastasis. I say apparently because of course the question immediately arose how his doctors could have been unaware of this widely disseminated cancer, which in all likelihood has been growing for years, and whether there was a “cover-up”. We know which group is running with the cover-up hypothesis, and conversely the folks who are lecturing that only conspiracy-theory nuts could imagine any attempted deception regarding some serious health issue in Joe Biden. Knowledgeable physicians have pointed out that the disease can be asymptomatic until it is widely advanced. Also current guidelines do not make a definite recommendation for routine PSA screening in men over the age of 70, and the word from the Biden team is that the former President was not having that test routinely measured as part of his annual physical. I would accept that assertion as truthful, for anything to the contrary would certainly be a serious deception, and sure to eventually be exposed. The argument is then made that, as leader of the world’s foremost national power, every reasonable investigation into the state of his health, including the simple PSA blood test, which despite limitations can detect early stage cancer, should have been done. The counter argument is that even though he is President, he should not be treated any differently than anyone else when it comes to general medical guidelines, and that testing in this situation is a decision made between the patient and his physician. To all this I would like to add something which I have not seen mentioned in the myriad articles so far published. His last physical (and perhaps earlier, though I didn’t check) reported that Biden had a peripheral sensory neuropathy of uncertain etiology, and that it is a contributing factor, along with degenerative spinal disease to his gait problems. While fairly rare, peripheral neuropathies can be a paraneoplastic syndrome—the result of a remote effect of an otherwise occult cancer—and there are published case reports of this type of syndrome as a presenting symptom of prostate cancer. Mr. Biden was of course evaluated by highly competent specialists in various fields including neurology, and not just by his generalist physician. It seems very likely to me that there was no overt cover-up of this malignancy diagnosis, but rather a concerted effort to avoid finding and documenting anything that could negatively affect his chances of re-election. This was beyond a shadow of a doubt the reality when it came to his cognitive decline. It is almost a certainty that Biden would never have done well on the most basic cognitive tests, and more comprehensive testing as a follow up would have revealed the extent of his dementia. Unless his personal physician was a complete idiot, he must have realized that; but you don’t document what you don’t test for. The absence of proof allowed for the continuation of plausible deniability, where the Biden camp and the media could dismiss the blatant signs of mental decline as “just another of ol’ Joe’s gaffes, Republican conspiracy theories, or malignant deepfakes”. It’s truly amusing to watch CNN’s Jake Tapper, who went to great lengths during the campaign to belittle and silence anyone pointing out Biden’s cognitive decline, now trying desperately to pretend that never happened, while doing his best to make money selling his new book about the nefarious efforts of others to cover up the truth. The US media bemoans the public’s evaporation of trust in them, but the cause resides directly at their feet—how many times do they imagine they can aggressively lie and distort facts, all the while proclaiming themselves to be the golden protectors of truth, yet still be taken seriously.
While we are on the subject of cancer I am calling attention to recent article in Nature regarding an association of a particular mutagenic chemical produced by certain strains of E.coli and early onset colon cancer. You are probably aware of the increasing rate of colorectal cancer (CRC) in young people in various areas around the world, including an 11% increase in the US over the last 20 years. Some strains of E. coli produce a chemical toxin, colibactin, which causes characteristic mutations in colonic epithelial cells, and the DNA sequences which code for this protein can be measured in CRC tumor tissue. These authors looked at specific colibactin mutation signatures in the tumors of a large number of patients, and found a very strong association with early onset tumors, and very little correlation in people with the classic later life onset CRC. Using some mutational rate statistical analysis they determined that the strongest correlation suggested exposure to high colibactin levels during early childhood. Other studies have shown some correlation between a “Western” diet high in meat and processed foods and colibactin exposure. Not everyone with higher colibactin levels is destined to get cancer, but a hypothesis is emerging that environmental factors may favor a person becoming colonized with the specific toxin producing E.coli, and colibactin in the presence of a Western style diet may be more likely to lead to cancer. Colonization with this bacteria is likely multi-factorial including genetic susceptibility, diet, breast feeding, antibiotic exposure during childhood altering the normal gut floral, immune response, and others. There is a comparable situation for chronic exposure to aflatoxin increasing the risk for hepatocellular carcinoma. There the toxin is produced by certain mold species which grow on food products in regions with primitive food storage practices. Mutagenic toxic from without, verses toxin from within. Lots of correlation studies are meaningless, duplicative, and a waste of time and money—but some give critically important clues to real causation. So skip the bacon, salami and bratwurst, and dive into that salad, organic kale and berries. Geographic and age variations in mutational processes in colorectal cancer https://doi.org/10.1038/s41586-025-09025-8

I pointed out in a prior post that tuberculosis must be the top infectious disease killer of all time. It didn’t win that title by causing sudden massive pandemics, like bubonic plague, influenza or COVID; tuberculosis is a stealth player, endemic in our species for millennia, and steadily grinding out a yearly death toll of staggering proportions over the centuries. Of course its impact is far greater in less developed countries with crowded, poor hygienic conditions—but that unfortunately is a still a wide swath of humanity, and approximately 1.7 billion people are currently infected with TB. The majority of individuals who become infected don’t die (otherwise TB might have succeeded in wiping out our species), but perhaps 10% of the approximately 10 million new infections every year will develop progressive disease, especially in the few years immediately after infection, with a resulting 1.2 million deaths a year. BCG vaccine for tuberculosis has been available for almost a century and is widely used around the world as a universal childhood vaccination. The effectiveness of BCG has been questioned for years; but a large systematic and meta-analysis study in 2022 provided good evidence that it is fairly effective in preventing infection in children age 5 and under, but that protection did not continue beyond that age.
Infant BCG vaccination and risk of pulmonary and extrapulmonary tuberculosis throughout the life course: a systematic review and individual participant data meta-analysis. https://www.thelancet.com/journals/langlo/issue/vol10no9/PIIS2214-109X(22)X0010-7
Protection in early childhood is very important because this age group is highly susceptible to the most severe and frequently fatal manifestations of TB, meningitis and miliary (disseminated) TB. The logical question to ask is whether revaccination of teenagers would boost the protective effect, since in countries with an extraordinarily high prevalence of TB like South Africa, this age group can have yearly infection rates of up to 10%. The study has been done and now published in the NEJM as a double-blind, randomized, controlled experiment vaccinating teenagers (who have no prior TB infection) and following the vaccine and placebo groups of 1800 people for 30 months. The results were disappointing and showed zero vaccine efficacy. Why the vaccine would provide protection in the youngest age group but not in adults is certainly perplexing, but a good reminder that seemingly logical approaches and common practice in the realm of medicine often don’t withstand the scrutiny of a randomized, controlled trial.
BCG Revaccination for the Prevention of Mycobacterium tuberculosis Infection. Published May 7, 2025
N Engl J Med 2025;392:1789-1800
DOI: 10.1056/NEJMoa2412381
In other vaccine related news the FDA and CDC issued a pause on the use of chickungunya vaccine Ixchiq in persons over the age of 60. This a live vaccine which perhaps few of you recognize, but it was approved in 2023 for the prevention of a viral disease clinically similar to dengue. The pause comes after reports of 17 severe adverse reactions, including 2 deaths, among the 80,000 doses given around the world. While there are always questions about whether a vaccine is responsible for unexpected side effects in post marketing experience, a look at the clinical trial data which led to FDA approval shows that 1.6% of vaccine recipients experienced what was described as severe prolonged chickungunya symptoms, verses none of the placebo group. Two vaccine trial recipients required hospitalization and some had prolonged symptoms interfering with normal activities for over 30 days, symptoms typical of the actual disease. That unusually high number of serious adverse events during the trial was most certainly vaccine related, and one could have predicted that a very high frequency of severe side effects would be seen with its “real world “ use. It is surprising to me that this vaccine was approved in the first place, and it appears destined for limited use or withdrawal from the market.
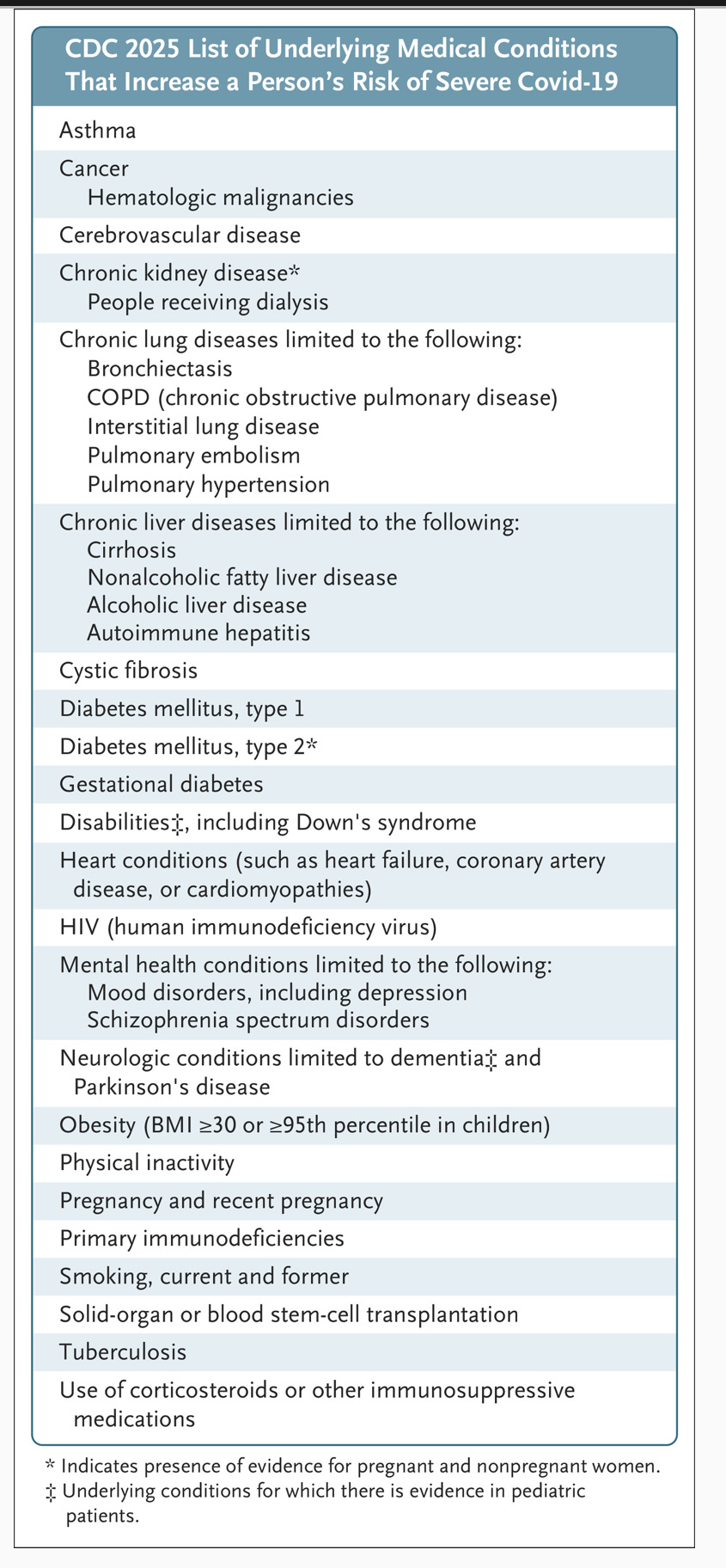
I mentioned in a recent post that the FDA vaccine advisory committee appeared likely to modify their recommendation for routine universal COVID vaccination to targeted high risk groups. The FDA has just indicated in a NEJM commentary that booster vaccinations going forward will be recommended for those over age 65 and those with the CDC defined conditions of increased risk. This would bring the US into close agreement with the rest of the developed world and especially Europe. I came across a piece just a few days ago suggesting rather hysterically that the new guidelines will not include pregnant women, but they are clearly included in the CDC list defining persons at increased risk, and the following CDC chart was included in the FDA commentary. Unfortunately the current state of American’s health suggests an enormous number of folks under age 65 will qualify.
One of the arguments made in this FDA communication is something I have long been writing about—having an official vaccine recommendation which is out of sink with the rest of the highly industrialized world, not supported by any current scientific evidence, and accepted as logical and believable by only a very small proportion of the population, is a contributing factor to more generalized vaccine distrust. The following is an excerpt from the NEJM FDA commentary, with my highlighting added.
There may even be a ripple effect (from the prior COVID booster recommendations): public trust in vaccination in general has declined, resulting in a reluctance to vaccinate that is affecting even vital immunization programs such as that for measles–mumps–rubella (MMR) vaccination, which has been clearly established as safe and highly effective. In recent years, reduced MMR vaccination rates have been a growing concern and have contributed to serious illness and deaths from measles.
I’m not sure new FDA Director Dr. Marty Makary ran that one past RFK Jr., but I don’t expect Dr. Makary to alter his scientific opinions to satisfy anybody else. The position paper also details plans to subject future vaccines, including COVID boosters, to rigorous randomized controlled trials, with realistically important clinical outcome objectives.
I’m wondering how long it will take for social media to light up with expressions of support and sympathy for the antisemitic lunatic who murdered a young couple at our capital’s National Jewish Museum. My bet is there will be a good overlap with the people who cheered the cold blooded murder of the United Healthcare CEO. If you find my posts useful, please hit that like button, subscribe and forward this to a friend. As a special bonus this week you can use the button below to message your favorite news person and express appreciation for their work.