
The last edition of Clear and Present Thinking was about the desire to live past 100. I have a follow up on that based on an August paper in Nature Aging. This research took a cross section of people of different ages and measured just about everything we can measure chemically: the RNA being transcribed (hence the active genes), hundreds of proteins, chemical metabolites, immune function and cytokines, glucose metabolism, inflammation, the composition of the gut, skin and oral microbiomes. Lots of statistical shenanigans, which I have to take their word for, and a plethora of very pretty charts show that aging is not a linear process, but that there are two ages where bursts of accelerated aging occurs pretty dramatically—the first around age 44 and the second starting at age 65. Those of you old enough to have crossed those portals might be thinking, “Yea that’s about right, and how much did this research cost?” It is nice to have some scientific validation of what your own body may have whispered, and hopefully down the line the mass of information here will be put to some practical use.
“Nonlinear dynamics of multi-omics profiles during human aging”https://www.nature.com/articles/s43587-024-00692-2

The summer COVID wave is still fading, RSV has not yet picked up, and the Flu season has not started in earnest yet. It does look like COVID variant XEC will take over as the viral holiday treat this year, but you just never know with this virus what might be lurking around the corner. Let’s take a look at some vaccine data just published by the CDC, and their recommendations for vaccinating seniors over 65.
Several days ago the CDC’s National Center for Immunization and Respiratory Disease published the most comprehensive data to date looking at vaccine efficacy in the more recent Omicron era. Because there is so much built up immunity to the SARS2 virus by now, the only metric that has any real meaning is comparing the vaccine efficacy over time of people who took the most recent COVID vaccine verses those who did not—irrespective of prior vaccination or infection history. Out of the many charts and graphs presented in the CDC slide deck, the following one is very instructive.
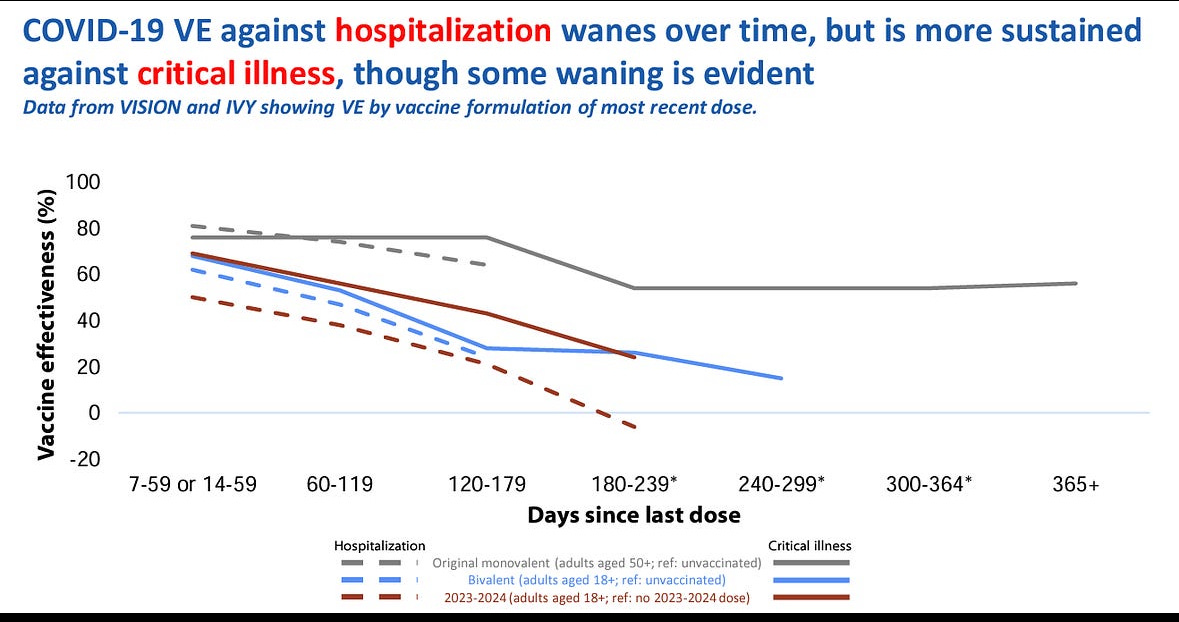
The dashed red line shows the vaccine efficacy of the most recent 2023-3024 COVID shot in preventing hospitalization over time. In other words, it shows the relative proportion of hospitalizations of people taking that vaccine verses not. As you can see, shortly after taking it the efficacy was about 50%. By 4-5 months there was no difference between the two groups. Protection from “critical illness”, shown by the solid red line, fared a little better, with protection at 4-5 months in the 30% range. The data doesn’t go out far enough to let us know at what point that protection is nil. It’s important to understand that the vaccine today is not performing much less efficiently than the original version—but that it is being compared to people who didn’t take the most recent shot, and have a great deal of pre-existing immunity. Vaccine efficacy today is the “frosting on the cake”, and it’s pretty thin at this point.

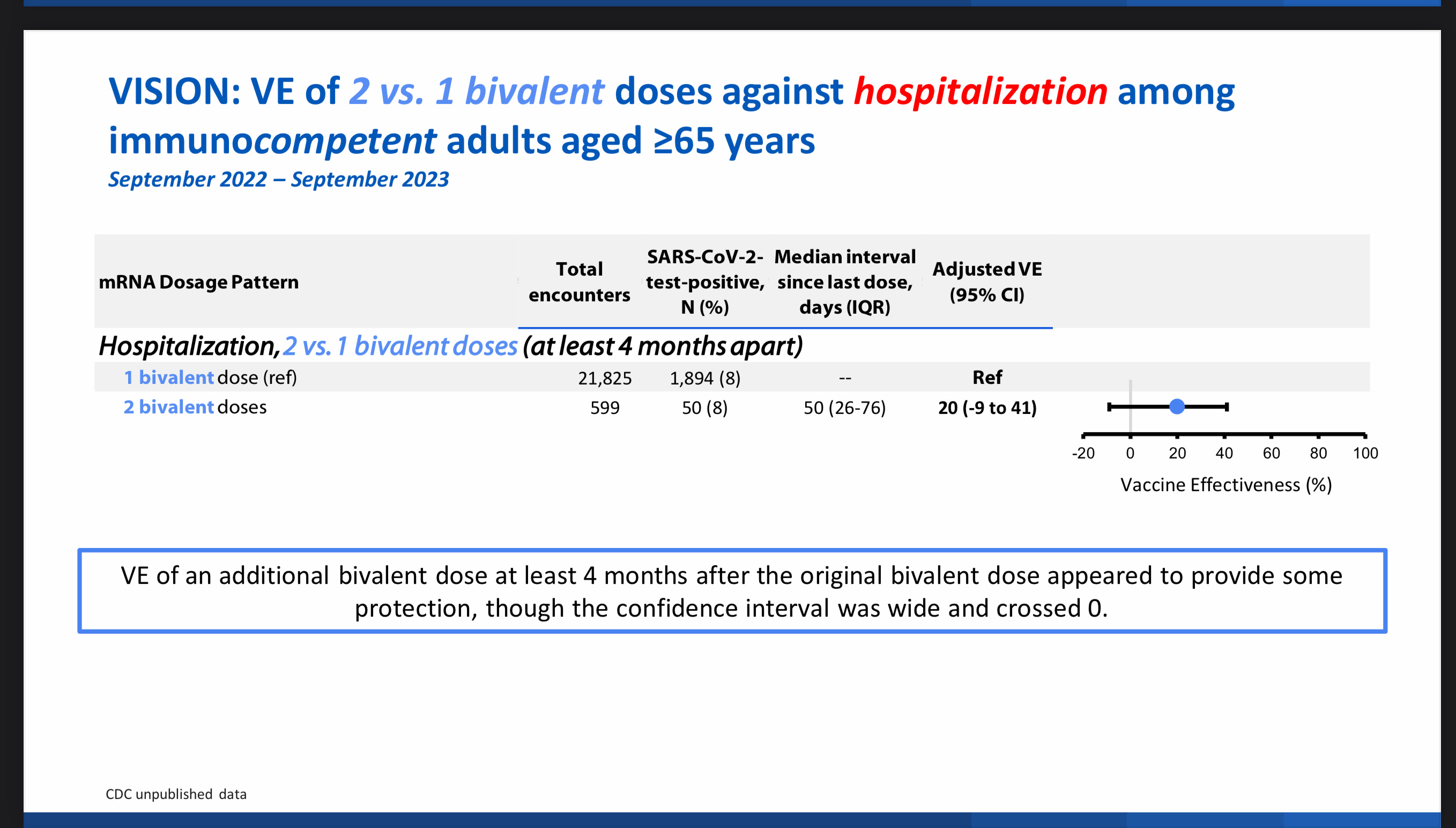
The CDC is responding to this data by recommending yet another COVID vaccine this spring for those folks over 65 and the immune compromised. They are effectively enshrining a recommendation for twice a year COVID vaccines in the over 65 age group. We have never given a vaccine with this frequency before; is there data to support this approach—or just the feeling that if the protection from hospitalization is gone in 4 months let’s give another shot. Protection from Influenza virus vaccination also declines within a few months of getting the shot, and if you take it early when the big pharmacy chains start pushing it, that can mean your protection is already waning right at the height of Flu season. Legitimate evidence that this twice a year COVID shot is worthwhile would of course mean comparing a cohort dosed twice against those receiving a single yearly dose. The CDC gives us the data from this past year on that very issue, as seen in the following chart. It shows VE (vaccine efficacy) for 2 doses given during the year, verses a group receiving only 1 dose. The numbers were small, with only 600 people evaluable in the double dose group. (No big surprise there). Look at the confidence interval as a result—the VE might truly lie anywhere between -10% and 40%. In my opinion this is hardly convincing evidence to recommend an unorthodox vaccination schedule to the whole population over age 65. Just as an aside on the issue of studies showing a possible negative VE. It has been erroneously seized upon by the entrenched COVID anti-vax group as evidence that the vaccine can make you more susceptible to infection, or more severe disease. That of course is nonsensical based on everything we currently know about vaccine science and immunology. The phenomena of a negative VE is also dismissed by some very pro-vaccine advocates as just a silly statistical aberration which should be ignored since it’s fodder for the anti-vaxers. The reality is that behavior of the individual receiving the vaccine factors into the “real world” evaluation of VE. If the vaccine is only marginally effective, and the recipient now feels emboldened and protected, (maybe they heard a nice elderly gentleman tell them from a prominent podium that if they take the vaccine they will not get COVID, and they won’t pass it to another person) the vaccine recipient may alter their behavior, and enter into more frequent exposure to the virus. The group of not recently vaccinated, may feel a bit unwary, restricting their activities and potential exposures a bit, and thus can easily be seen to contract less disease in this type of low vaccine efficacy situation. Or at least that is what I think—contrary opinions always welcome.
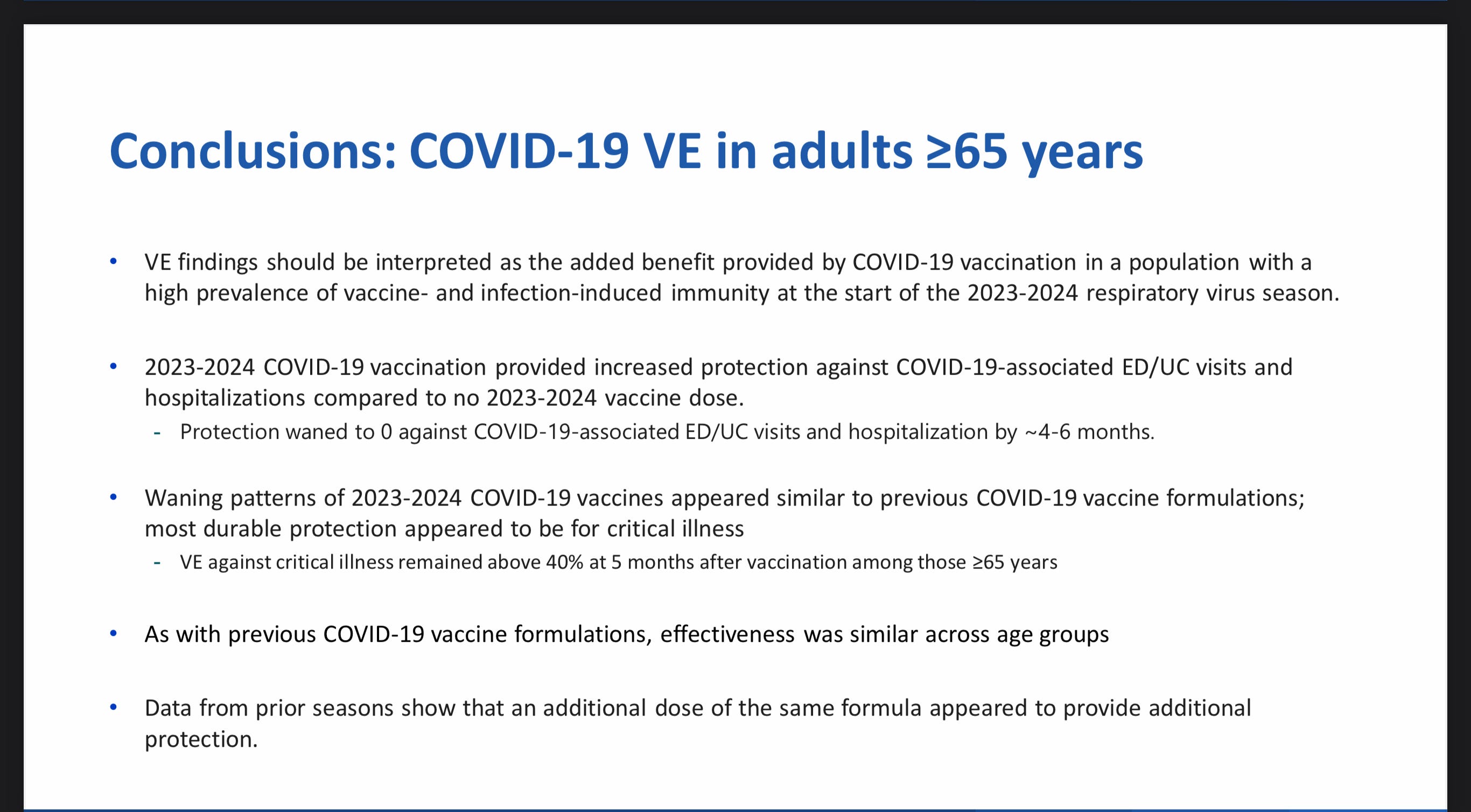
I am including a link to this week’s CDC data dump slide deck on this issue for those wanting a deeper dive into the weeds. Yes, the data do continue to show that protection from critical illness remains more durable at 6 months (at about 40%), than protection from hospitalization. At this stage of the Pandemic game the people truly at risk for critical illness and death are the very elderly, and folks with severe underlying medical problems. The following is the summary slide from the CDC presentation.
https://www.cdc.gov/acip/downloads/slides-2024-10-23-24/04-COVID-Link-Gelles-508.pdf
This is the potpourri section, so expect some quick observations and opinions without much science: 1. Rachel Walensky just received IDSA’s Anthony Fauci Courage in Leadership Award. I’ve written a great deal over the course of the Pandemic about how national officials inadvertently contributed to the distrust of Public Health and Science in general. Anyone who has been reading these pages for a length of time knows exactly how I feel about Rachel Walensky’s performance as CDC Director—both in the substantive decision department, and in the communication realm. Despite hiring outside consultants to improve her communication skills, I think Dr. Walensky realized that a huge segment of the populace shared my conclusions, including many folks in academia, and she decamped back to Harvard as quickly as possible trying to save face. To begin to restore confidence in Public Health, the field needs to vocally admit what they got wrong, as well as try to communicate clearly what they positively achieved. Giving this award to someone who got so much wrong seems to me like giving Margery Taylor Green the AOC award for Excellence in Political Science, or George Santos and Eric Adams sharing the Robert Menendez Honesty in Government Award.
As you probably know there was a case of polio in Gaza for the first time in 25 years, and circulating polio virus found in the waste water. One case is considered an outbreak since it implies there may be about 200 other infected people who are asymptomatic, or minimally ill with symptoms that never get diagnosed as Polio. Of course, the war time conditions are a major factor favoring spread of this disease, but now we know which Polio virus paralyzed the 1 year old child, and of course it is the cVDPV2 (circulating mutated vaccine derived virus). Why do I say, “of course”, because there has been no wild type natural Polio virus there for a quarter century, and certainly nobody is traveling into Gaza recently for vacation. Introduction from Egypt though is possible. Egypt was declared Polio free in 2004, but guess what—the country had an outbreak of the vaccine derived virus in 2021 and again in 2023. I will be interested to see if this current isolate exactly matches the mutated Egypt vaccine strain.
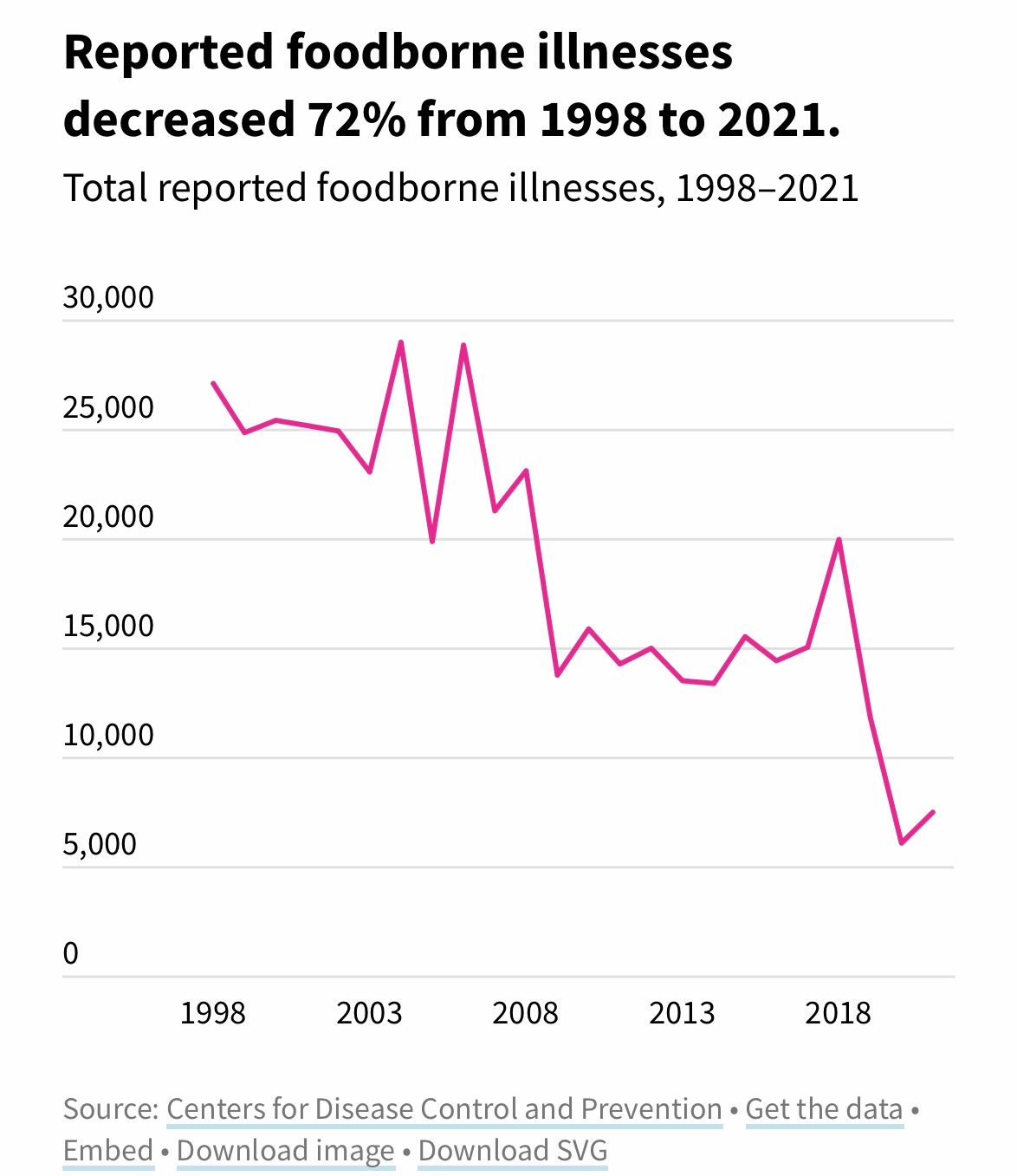
Revisiting the issue of the safety of the food supply—you have no doubt heard that MacDonalds has joined the ranks of establishments linked to contaminated food causing an outbreak of illness. This time it is E.coli infections from the quarter pounder in 13 states, with 75 people confirmed affected so far. The CDC estimates that almost 48 million people get sick from food borne illness every year, with 128,000 hospitalized and 3,000 deaths. The estimate of 48 million seems incredibly high, but the vast majority of cases are mild, undiagnosed and under reported. Recent high profile stories might lead you to believe that this problem is becoming more common; however, CDC statistics show a fairly steady decrease in reported cases over the last 20 years.

Israel just struck back at Iran in retaliation for the recent massive missile and drone attack. It was by all accounts a surgical and limited attack, designed to seriously weaken their air defenses and offensive weapons production—but not enough to make their turbans spin completely out of control. This should induce a temporary lull in the tit-for-tat strikes as the Mullahs contemplate how wildly inferior their Russian armaments were against more sophisticated equipment. They will be thinking that they are even more exposed now with their inadequate air-defense batteries blown up, and weighing the pros and cons of a future Israeli regime toppling strike, verses the 40 virgins in Heaven should they choose the martyr route. The images of Yahya Sinwar throwing a stick at an Israeli drone seconds before being blown up, the high tech wizardry of the Hezbollah beeper episode, and the inability of Iran to thwart this Israeli attack, even though details were likely leaked to them in advance, is not a good look in the Arab world, where Iran has become more isolated and despised. The Mullahs can still do crazy unpredictable things of course—so ahead of the US election I advise buying
American weapons makers and gold.
Thanks for your attention today. Please forward these pages to friends and associates, and hit the like button which is hard wired to my dopamine receptors. Don’t be afraid to express yourself, this is a cancel free zone, even if it is heavily monitored by the FBI, CIA and NSA. Don’t forget to vote and Rock the Casbah.
Love your blog. Thirty years ago I remember having a two-day discussion with my brother-in-law ( a physician) about the fact that our country has virtually no public health system. The CDC sits on their high throne in Atlanta and publishes. Nothing else. And to give Walensky an AWARD?? Oh please. Smoke and mirrors. Thanks for your great articles. The bonuses are the chuckles I get when I read them.