

CDC: Start Making Sense
Does COVID really need our help in mutating?

There’s an old Talking Heads live performance film from the early 1980’s entitled STOP MAKING SENSE. I have this nagging feeling that people at the CDC may have viewed it back in the day, and taken the message to heart. You might suppose I’m referring to the recent approval of the new COVID mRNA boosters for everyone over the age of 6 months. The wisdom, or lack thereof, of that decision has been sufficiently debated by experts and pundits over the last two weeks, and you have probably formed an opinion on the issue. One of the members of the ACIP committee William Shaffner MD, (Vanderbilt Professor of Medicine and Preventive Medicine, as well as Medical Director of the National Foundation for Infectious Diseases) said he was initially in favor of a more restrictive approach—that the booster be approved for people of ages and medical conditions placing them at actual risk for serious illness; but his mind was changed by other members of the committee arguing that they should approve it for everyone so insurance companies would be forced to cover it for absolutely anyone wanting to receive it. I suppose that’s an example of the Science we are supposed to be following.
If you live in New York, the northeast or mid-Atlantic region it might seem like a whole lot of folks have COVID right now, and you would be right. It does appear, based on waste water viral RNA, that this wave of disease has peaked, and is just beginning to fade a bit in that region, and areas of increasing activity have moved to the upper midwest. Here is a nice graphic showing COVID disease activity (based on hospitalizations around the country as of September 16th).
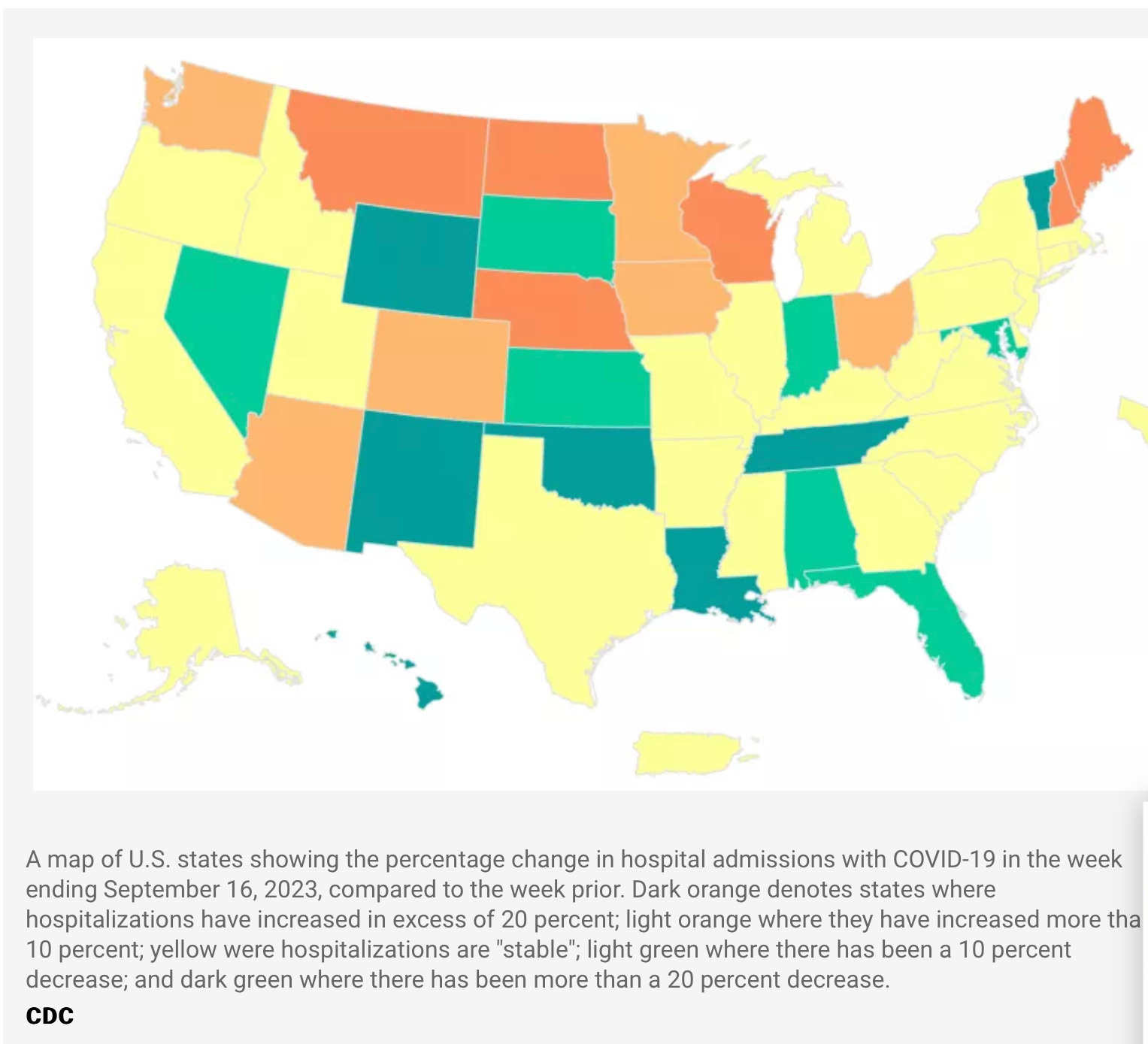
Some weeks ago I predicted that total US COVID hospitalizations would reach 20,000 per week, which they did; and this week for the first time since June, hospitalizations slipped downward a bit to the 19,000 range. As far as I am concerned that signals the current summer long wave is decreasing for the country as a whole. Many people who have had COVID in the last days, weeks or months are legitimately wondering when, or if, they should take the new booster shot. The CDC officially states that you can take the new vaccine, “as soon as your COVID symptoms have resolved”. They go on to say, “but you may want to wait up to 3 months” after an episode of COVID. There was a time when I would have expected the CDC to be consistently handing out advice that makes sense scientifically, but that ship seems to have sailed. The scientific evidence is quite clear that your response to the vaccine is very significantly reduced when you are dosed shortly after an episode of infection. Right after a bout of COVID your neutralizing antibodies are sky high and: 1. You don’t NEED a booster and 2. Your immune system will BARELY respond to it. We knew early on that the longer the interval between the first dose of vaccine and the second, the higher the antibody response following the second shot, and the longer the antibodies remained elevated. Immunologists and experts in vaccine science know this, and various experts have recently opined that you should wait 3 or 4 or 6 months after infection to receive a booster. Nobody knows exactly how long is optimal based on any hard evidence—but my point is the CDC should not be telling people they can take a booster as soon as their COVID fever or other symptoms go away. Sure, you can perhaps take an antibiotic when you have a runny nose, or maybe some chemotherapy for a toothache—drugs you don’t need, won’t help you, and will have side effects—but the former premier epidemiological institution in the world should not be suggesting this. I have previously offered my opinion as to who even needs another booster dose at this time; and let’s just say that some extremely knowledgeable folks, like Professor Paul Offit, agree with me that basically healthy, previously vaccinated, then later infected people (even in their 60’s) have sufficient persistent T cell immunity to avoid any serious disease. There is room for disagreement of course, and isn’t it marvelous that perhaps we have progressed (?regressed) to a point where folks can disagree about issues related to the vaccine without resorting to ad hominem attacks and name calling? Perhaps future CDC decisions will also be called into question……
For those with more curiosity than my say so (always a good idea) here is a link to a paper in Cell detailing the experimental evidence which supports waiting after COVID infection for any further vaccination
Interval between prior SARS-CoV-2 infection and booster vaccination impacts magnitude and quality of antibody and B cell responses. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9513331/
The next item that made it to the mass media press this week was the story of Merck’s drug mulnupiravir (trade name Lagevrio) causing highly mutated COVID variants, and questions about whether this represents a risk. The drug works by substituting itself into the RNA of the virus as it is copied, and then subsequently when that chain is copied again it leads to huge numbers of mutations. The therapeutic model is that the vast number of such highly mutated virions will be lethally compromised and unable to function normally; the viral replication is shut way down, and the scale is tipped in favor of your immune system clearing out the virus. This week a paper appeared in Nature (I referenced this work earlier this year when it appeared as a pre-print) showing that strains of SARS2-CoV19 virus, extensively mutated by molnupiravir are found in the data base of strains collected around the world. I won’t go into the details (link to the paper will follow) other than to say there is a particular molecular signature typical of molnupiravir’s effect in these viruses, and the evidence is pretty clear they evolved in treated patients, and have had forward transmission to other individuals. This virus is mutating all the time, in every person who gets infected, so what’s the concern? First, the virus has an intrinsic rate of mutation at every site which is determined by the error rate of the RNA polymerase (the copying enzyme). By introducing molnupiravir we are massively increasing the mutation rate across the genome. It is true that almost all the subsequent virions are defective and at a dead end—but the Nature paper shows that not all of them are. Immune pressure from prior infection and vaccination has primarily selected for changes in the S protein (spike protein and the specific region that latches onto our cellular receptor, the RBD or receptor binding domain). You may recognize that as the phenomenon of “convergent evolution”, but there are many other areas of the viral genome that affect it’s ability to replicate after entering the cell, allow it to evade our early innate immune response, and various other functions of the virus which are tied to how virulent it is. What about immune compromised people with COVID who get treated with this drug? Their immune system can fail to clear the virus fully even though molnupiravir is decreasing the viral replication rate—so the infection can go on and on with billions of highly mutated viruses until something pops up which can still replicate, evolve further in the setting of inadequate immune response (we have seen this before with the monoclonal antibodies, which are now useless).
https://doi.org/10.1038/s41586-023-06649-6 A molnupiravir-associated mutational signature in global SARS-CoV-2 genomes
Is it a good idea to be accelerating the rate of mutation of regions of the viral genome which determine it’s ability to evade our immune system, or control it’s virulence? I don’t think so. I never thought molnupiravir was a good drug given it’s inferior effectiveness compared to Paxlovid (nirmatrelvir/ritonavir) —this new data showing forward transmission of drug mutated virus is a warning. I’m bringing back an old friend at this point to see what Dexter (aka Viral Creep) thinks about this.
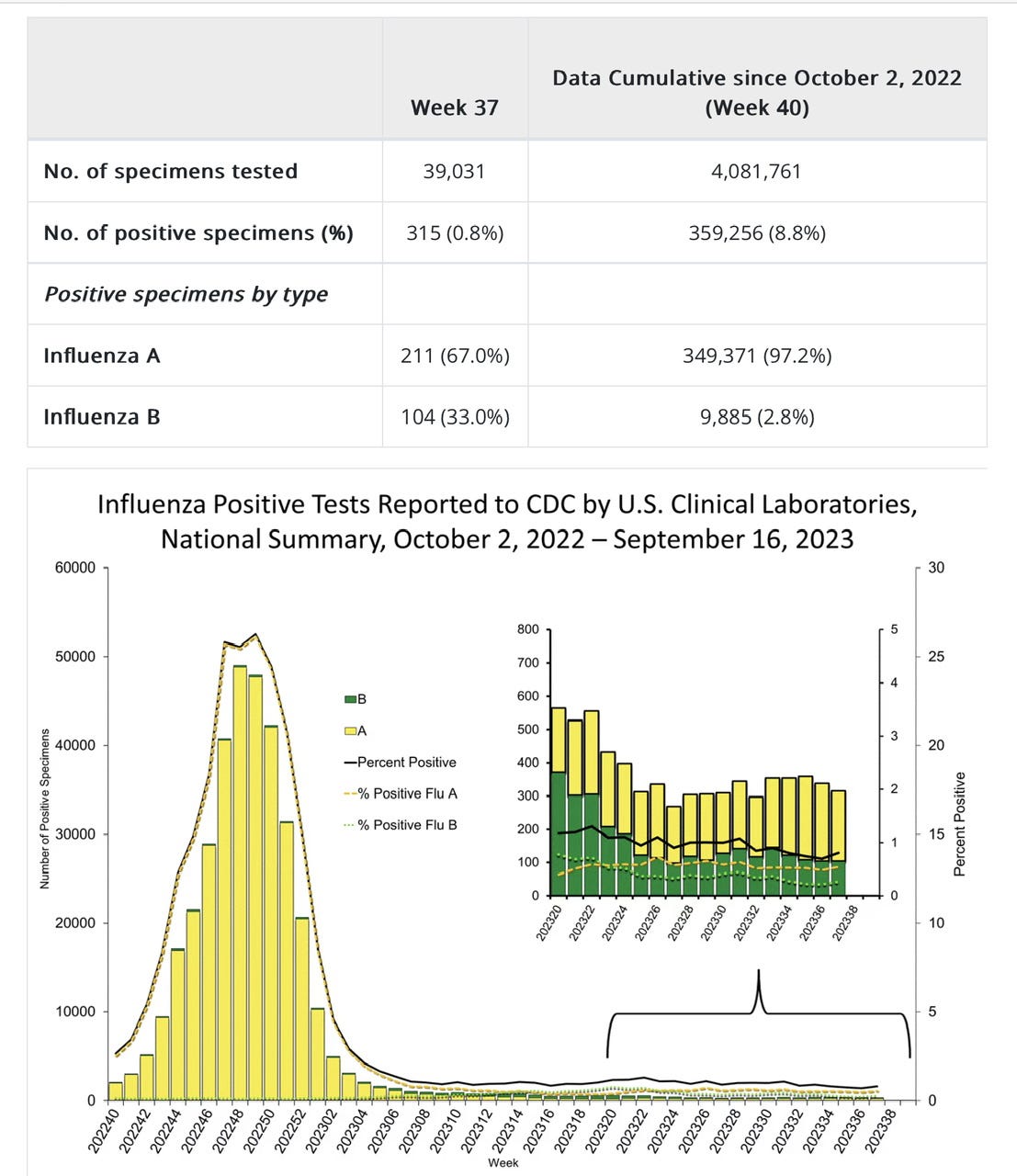
If you have been reading the tabloids you know about the “Triple Epidemic” of viral respiratory disease (Influenza, RSV and COVID) being predicted for the winter season. We used to be pretty good at predicting the seasonal patterns of some of the major respiratory viruses, but the Pandemic has caused a dislocation affecting the timing of Influenza, RSV and other viruses which is still persisting. Right now there is a huge outbreak of Influenza in Russia, and a more typical late summer outbreak in Hong Kong. The following graph shows there are still extremely low cases of flu in the US—all those people in NY sneezing, coughing and claiming to have the flu are mistaken. Note especially the very low % positivity rate. If you choose to take a flu shot, as I do every year, it would be reasonable to delay it well into October, so your antibody levels are still adequate later in the winter. Travel, access to vaccination, high risk medical conditions and immune suppressing treatments of course are wild-cards favoring earlier vaccination. Some good news is that the strains of Influenza being reported from the Russian epidemic seem to match well with the stuff which will be going into your arm.
The news cycle changes faster than the Senate dress code these days. In the twinkling of an eye Chuck Schumer altered the dress code so Senators could appear like the drunk cousin of Sasquatch, only to have the entire Senate (in the only example of unanimous bi-partisanship in recent memory) vote for serious working business attire. If only they used those suits to accomplish some serious business. This week we also learned that inflation has so devalued the US dollar that when bribing a US senator one must bring gold bars in addition to packets of unmarked bills. Personally I have to agree with all the senators demanding Menendez resign—not because he was selling influence to the highest bidder, that seems to be quite routine in Washington DC. these days. It’s rather his inept, bush-league approach to bribery which gives me no confidence in his ability to help lead the country. Remember the like button dispenses Gold bars with traditional Egyptian blessings in Spanish, and is directly tied to my dopamine receptors. Sharing this post is most appreciated.
Great article! Love the closing humorous commentary!