Connecting the Dots
More Inconvenient Facts


New data is emerging quickly on the immunologic effectiveness of the bivalent boosters in humans. As you recall, the CDC charted the course to requiring Pfizer and Moderna to produce the new boosters containing reduced doses of both Wuhan and BA.4/.5 Spike RNA, and the FDA cleared the way for their EUA use based on the slimmest of mouse data. Two weeks ago we got the first glimpse of human clinical data with Pfizer’s press release stating that the bivalent vaccines produced “higher” antibody levels against Omicron BA.4/.5 than the old monovalent booster. No quantitative results or details of the study were made available. Pfizer went further, and stated that based on these results we could expect improved protection from the new boosters. In the last several days independent research groups from Columbia University and Harvard have released preprints both showing no significant difference in the levels of NABs (neutralizing antibodies) produced by the old boosters and the new formulation.
Antibody responses to Omicron BA.4/BA.5 bivalent mRNA vaccine booster shot, Quinn Wang, et al. https://www.biorxiv.org/content/10.1101/2022.10.22.513349v1.full.pdf
Immunogenicity of the BA.5 Bivalent mRNA Vaccine Boosters Ai-ris Y. Collier, M.D., et al. https://www.biorxiv.org/content/10.1101/2022.10.24.513619v1.full.pdf
Put these studies together with the data we highlighted last week, showing the bivalent boosters primarily stimulate an increase in pre-existing memory B cell antibodies against BA.4/.5 (created by the original Wuhan vaccine or infection)—and the picture emerges that very likely immune imprinting is at work, and the new boosters offer no real advantage. Immune imprinting describes the situation where the immune system becomes “fixated” on a particular antigen after multiple exposures, and when exposed to a new antigen which is very similar, tends to ignore subtle changes and rev up the prior memory response, at the expense of making brand new unique antibodies. Of course you have to ask yourself, who am I more inclined to believe at this point; the independent researchers at a number of University labs, or the guys making 30-40 billion dollars a year selling a now less than stellar product? Some people in the camp I will label, The government can do no wrong—as long as it’s my political party—are saying, “so what”? Beyond the enormous amount of money spent on purchasing the new boosters, there are other considerations. There are many people who were vaccinated and boosted with Wuhan, but appear to be holding back on getting the new bivalent boosters out of concerns over the lack of human testing. These are not vaccine deniers, or belatedly buying into out-right lies about the vaccine, but are perhaps simply exercising a common sense approach, and looking at declining COVID case numbers in determining their perceived risk. Then there is the issue of further imprinting our immune systems to a variant BA.5, which already appears to be declining, and just may vanish in the very near future as the even more adroit antibody escape mutants BQ.1.1, BA.275.2, or XBB take over. Another consideration is that we have never experimented with such frequent vaccinations against a rapidly evolving virus. Will immune tolerance or fatigue become an issue, along with the immune imprinting that seems to be occurring. Rachel Walensky, the CDC director, contracting COVID two weeks after receiving her bivalent jab isn’t exactly a confidence booster, and couldn’t have come at a more inopportune moment.
We have been frequently assured by our Public Health authorities (the CDC, Dr. Fauci, the White House COVID task force, among many others) that even though the vaccines have essentially lost the capacity to prevent infection, that they are continuing to provide very good protection from serious disease—even if that protection is, to quote Anthony Fauci, “slipping a bit” now. A good deal of the data backing up those assertions was generated during earlier waves of the Pandemic, and not during the Omicron era. One of the biggest failings of the CDC has been the very slow, spotty collection and analysis of epidemiological data during the Pandemic. We have been forced to look elsewhere, to Israel, the UK, and others, to get a sense of what’s coming next, vaccine efficacy against variants, and how frequent are reinfections. In the October 21 issue of MMWR, the CDC published an analysis of data looking at the efficacy of the RNA vaccines in preventing hospitalization. I think we should review theses findings and then connect the dots….to see the elephant standing in the room.
Effectiveness of Monovalent mRNA Vaccines Against COVID-19–Associated Hospitalization Among Immunocompetent Adults During BA.1/BA.2 and BA.4/BA.5 Predominant Periods of SARS-CoV-2 Omicron Variant in the United States — IVY Network, 18 States, December 26, 2021–August 31, 2022
MMWR Weekly / October 21, 2022 / 71(42);1327–1334
It’s certainly worth reading the report, and I am only going to concentrate on the data relating to BA.4/.5, since that is what we have to confront today, the previous variants being only of historical interest.
During the BA.4/BA.5 period, VE (vaccine efficacy) estimates of 2 doses 14–150 days and >150 days after the second dose were 83% and 37%, respectively; VE estimates of 3 doses 7–120 days and >120 days from the last dose were 60% and 29%, respectively. VE of 4 doses 7–120 days after vaccination was 61%. (No data provided beyond 120 days) …. Among immunocompetent adults hospitalized within the IVY Network in 18 states, a monovalent booster dose of mRNA COVID-19 vaccine had limited overall effectiveness against hospitalization caused by currently circulating SARS-CoV-2 Omicron variants, likely because of waning immunity. Waning protection against COVID-19–associated hospitalizations was observed with either 2 or 3 doses of mRNA vaccine during the BA.1/BA.2 period with similar emerging trends during the BA.4/BA.5 period.
The protection against severe disease in this Omicron era falls from 60% immediately after the booster (the period of highest antibody levels) to 29% by 4 months. Not very good, but a little better than nothing. If you are over 65 or compromised, you just might be one of the folks it keeps out of the hospital. Let’s connect the dots now. The Administration, the CDC and the drug companies are all signaling that you will be getting a yearly COVID booster every fall. We just reviewed the evidence pointing to the bivalent boosters not looking perceptively better than the original vaccine. A short time frame will give us clinical vaccine efficacy data, and a comparative look at the efficacy of the European Union solution boosters, which target BA.1 instead of BA.4./5. If you get boosted now, you need to be aware there is an excellent chance that your increased protection will be largely gone by the dead of winter, and the peak of respiratory virus season when we huddle indoors, and breathe each other’s exhaled air.
The hard sell on the bivalent jabs is beginning in earnest now, since uptake of the new boosters has been sluggish at best, with only 14 million doses administered. For comparison, 111 million people in the US have received a previous booster. Everyone from Hollywood to sports stars and Big Bird will be hawking them, in all media formats. President Biden said this week that almost every COVID death this winter would be preventable if people just get the new booster. That’s nonsense of course, and you can choose to call it a lie, disinformation, or just another gaff from Ole Joe depending on your inclination. You know I’m in favor of high risk individuals getting boosted, but one size does not fit all, and everyone will need to use the data available to make their own informed decision. One thing I strongly disagree with the CDC about is the recommendation to get boosted as soon as two months after a prior booster or infection. There is plenty of evidence that boosting too soon after a prior exposure will attenuate the antibody response, so you won’t get the bang for your buck. (Ok the shots are still free, but that ends with this round). If we accept that the vaccines are not really providing significant protection from infection, and that protection from severe disease is still fairly stable at 2 months—where is the logic of boosting at that juncture and thus reducing the level of NABs increase you realize?
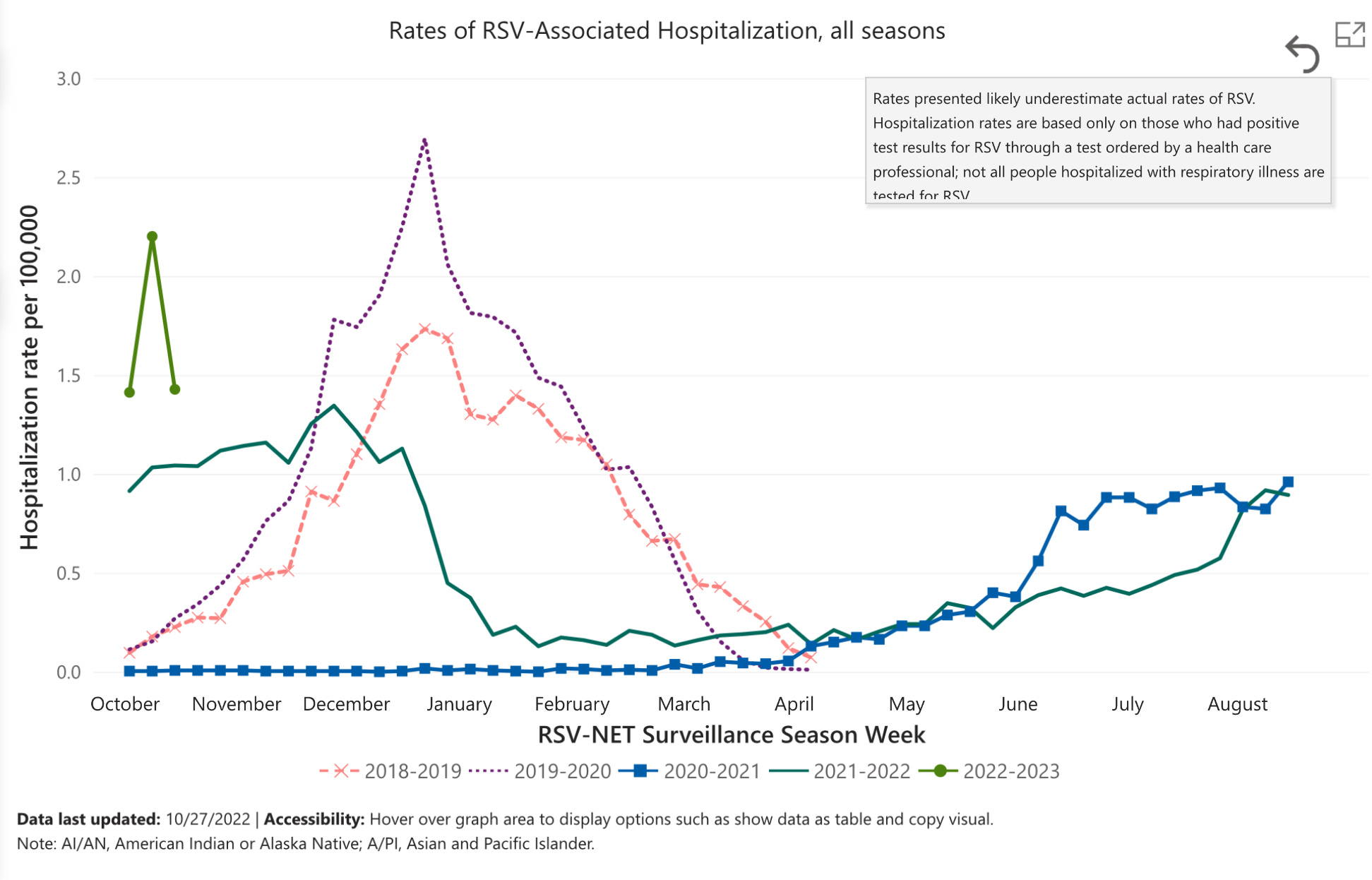
Next I want to revisit a topic I discussed two weeks ago, and that is the Pediatric RSV and other viral disease epidemic. It is getting worse, and is of great concern since we are not close to the usual historic peak period of December through January. The following chart is from the CDC RSV-Net surveillance system. As you can see on the left, we are at dramatically higher RSV hospitalization rates than usual for this time of year. The graph also makes very clear the astonishing absence of RSV disease during the lockdowns of 2020-2021, and the unusual uncoupling of the disease from its historic temporal pattern of winter peak, during the summer of 2021. Right now pediatric hospital beds are 75% filled (an unusual situation for this time of year), and we have yet to see the full impact of Influenza, and whether RSV will continue to escalate along its usual trajectory.
Finally I’d like to highlight how low tech observations, and our own powers of reasoning, can sometimes give clues to the bigger picture—without a virology or immunology lab in the basement. Social media reports noting complaints on Internet sales sites about scented candles having no smell led one college professor to collect the data, and find that indeed the number of these complaints directly paralleled, and slightly preceded the number of clinically diagnosed COVID cases in the region. On a recent visit to family in North Carolina I was surprised to see that the CVS shelves of pediatric cold medication and ibuprofen were bare. My son immediately said, “I guess everyone’s kids must be sick”. Two days later we learned on the news that local schools were experiencing 30-40% absentee rates.
https://apple.news/ABmbKlC5yTqSOroK7tzP9dg Why did he suspect a COVID surge was coming? He followed the digital bread crumbs. NPR
Happy Halloween to all the Trick or Treaters. Take my advice it’s still too soon to go out as a Corona virus. Investigate the facts, and use you own Clear and Present Thinking whenever possible. If you find these pages informative please send them to someone in your circle. Please comment, that is most welcome—as well as the like button, which gives me a small rebate from the IRS every time you use it.
Thanks Jeffrey! What about the duration of Natural immunity?? I am over 65, healthy, fully vaccinated with three doses of original vaccine, the third dose given at the end of March. Then I got Covid from an August outdoor wedding that moved indoors during a rain storm. I was told to get a booster 120 days after testing positive for Covid. Your thoughts?
I'm not a doctor, so thanks Jeff for always adding some comments (and humor) for the layperson as well.