

COVID Aftershocks
A new drug menace hits the streets

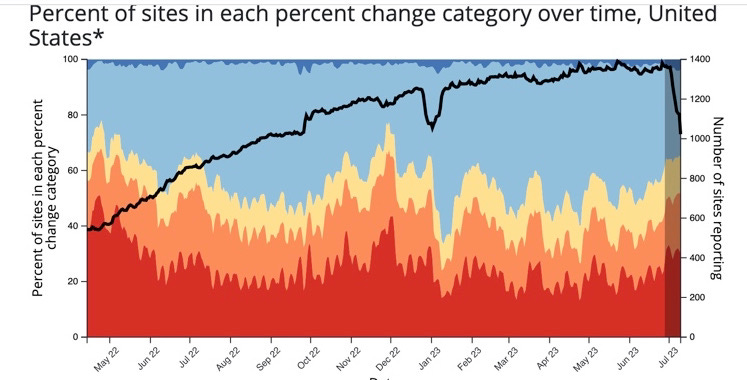
There are a lot of parallels between the 1918 Influenza Pandemic and the COVID-19 Pandemic. The H1N1 Influenza swirled around the world for 3 years and more before settling down into the typical endemic seasonal pattern. Like COVID, the second wave of H1N1 was worse in terms of mortality figures— and by COVID’s second wave we at least had the benefit of life saving vaccines. Successive waves of both viruses swept rapidly around the world, but as the 1918 pandemic petered out the pattern shifted to localized areas of high transmission, while other regions of the globe were essentially free of disease. That is exactly what we are seeing today. The US has had continued reduction in measured disease activity, while isolated regions of the world (Poland, Brazil, South Korea, Japan, and Vietnam ) are still experiencing high levels of COVID. Here at home, most people have basically forgotten about COVID, at least as judged by their behavior. There are exceptions, like the Harvard system hospital where they recently re-instituted mandatory universal masking after a nosocomial outbreak of COVID; or the White House decision to continue requiring masking and 6 foot social distancing only for people not “fully vaccinated”. That is perseveration in my opinion, not based on any sound scientific reasoning at this point in time. Last month the Centers for Medicare and Medicaid withdrew its requirement that healthcare workers get COVID-19 vaccinations, and many US hospitals have already dropped the rule. Despite the relatively low level of hospitalizations, 6000 in the last week, the virus is very much still with us as is evident from the following CDC wastewater graphic. The poop doesn’t lie, and the COVID is biding its time until the usual cold weather respiratory virus season. (The graph shows total number of sites reporting large increases in waste water COVID in red and large decreases in blue)
Let’s examine some of the Pandemic aftershocks. Long COVID sufferers are the most obvious; but we still know very little about this issue. Despite enormous numbers of studies and voluminous writings, it remains unclear how many people are affected, any concensus on the pathophysiology, effective treatment or prognosis for the long term sufferers. I find it a happy coincidence that among the hundreds of people I know who have had COVID once, twice or three times, that not one of them has complained about suffering from Long COVID—and I make it a point to ask. Beyond the lingering effects of the virus, there are the problems which appear to be the result of social policies adopted during the Pandemic. It will take years to fully measure many of the negative effects—but some are readily apparent now. Social isolation resulting from the lockdowns has been linked to increased rates of depression and suicide, untold, unquantifiable misery for elderly people separated from friends and family in nursing homes, and those facing the end of life alone. There is one constant in human existence, and one of the saving graces of the human condition is the dignity and comfort afforded by being surrounded and supported by loved ones at the end of life. As a society we should think long and hard about ever allowing this to happen again, especially on the recommendation of dubious or non-existent evidence.
Alcohol and drug abuse increased at dramatic rates during the Pandemic especially during the periods of lockdown. A US study in 2021 found that mothers of young children increased their alcohol consumption by a whopping 325% compared to pre-pandemic levels. While this finding was based on surveys, and was subject to recall bias, other studies looking at rates of hospitalization for alcoholic hepatitis have confirmed a serious increase in acute alcohol related liver injury. This representative study from a California hospital system published in the Journal of Gastroenterology and Hepatology, showed the following results for increases in alcoholic hepatitis admissions and deaths in 2020 and 2021 compared to 2019.
The number of cases increased from 131 in 2019 to 201 in 2020 and 215 in 2021 (53% and 64% increase, respectively). The number of young patients (age <40 years) increased from 30 in 2019 to 61 in 2020 and 71 in 2021 (103% and 136% increase, respectively) (p = 0.13). The number of admissions of women increased from 24 in 2019 to 55 in 2020 and 67 in 2021 (129% and 179% increase, respectively) (p = 0.026). Deaths during hospitalization increased from 20 in 2019 to 26 in 2021 (p = 0.674). The number of re-hospitalizations within 3 months increased 4.5 times from 18 in 2019 to 80 in 2021 (p < 0.001).
Soaring rates of alcohol‐related hepatitis in the latter phase of the COVID‐19 pandemic: A new normal? Published online 2023 Jan 13. doi: 10.1002/jgh3.12864
Given the dramatic increase in both recalled alcohol consumption and admissions for alcoholic hepatitis among young women, it’s not hard to picture mothers stuck at home with the stress of trying to care for young children (who should have been in school) while remote working, and having more socially isolated time to drink.
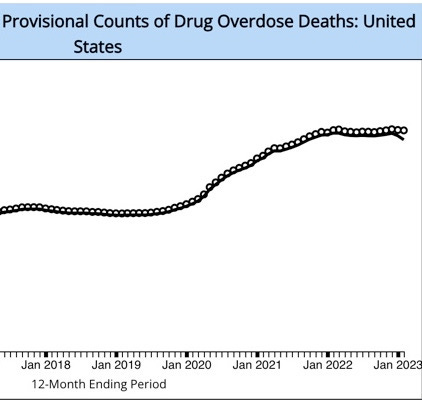
As far as drug overdose deaths are concerned, the story of the tragic increase accompanying the Pandemic is well known. We can’t tease out the the relative contributions of the societal lockdowns versus the dramatic increase in the availability of fentanyl flooding across our southern border, but the sudden increase in deaths coinciding immediately with the onset of the Pandemic, and well prior to the surge in fentanyl importation argues strongly for a result of social isolation and lockdowns. Here is a graph over time from the CDC showing an increase in OD deaths from 69,000/yr in 2019 to over 100,000/yr in 2020 and currently still 105,000/yr. The vast majority of the OD deaths are young people, and it is obvious that enormously more of these young folks died as a result of various government policies than from COVID.
Fentanyl is now being laced with Xylazine, a drug used in veterinary medicine for large animal sedation. The drug is an agonist of the alpha2 adrenergic receptor, which causes central nervous system depression, and in the peripheral nervous system causes intense vasoconstriction of arterioles and veins in the skin and subcutaneous tissues. The result of injection abuse of the two drug combination is to increase the rate of fatal OD, and to create horrific necrotic soft tissue lesions. (Skip picture which follows below if you’re not a medical professional). The combination goes by the enticing street name of Tranc-dope (which by coincidence is the Secret Service code name for Hunter Biden). It turns out Xylazine is not a scheduled drug in the US—cutting fentanyl with it simply means that it is cheaper and even easier to get. The Biden administration just announced a plan to attack the problem of Xylazine laced fentanyl. Given the success so far of any plan to address the pure fentanyl crises (if in fact there was one), I wouldn’t hold your breath. Billboards and bus advertisements for Tranc-dope with the following picture would be my contribution if anyone in Washington comes asking.

Another highly significant aftershock from the Pandemic, which I have discussed in prior posts, is the sudden marked drop in mathematics proficiency in junior and high school students. The Teachers Union, and various people who enabled their unscientific endless school closures, may try and insult your intelligence and common sense by pretending the the two are unrelated. California has the largest public school system in the country, and currently only one third of high school students perform at a satisfactory level on the state standardized mathematics test. Among students from poor families the statistic is 1 in 5. The situation in multiple other areas of the US, including New York, is similar. California has announced a 1000 page plan to improve mathematics instruction, which has been met with considerable criticism from multiple experts in the field. An extensive part of the plan is to make mathematics more “culturally relevant”, as a way of engaging student interest. My guess is that they will end up dumbing down the requirements of the state testing, and show resounding success in just a few years.
In other COVID related news, another study has shown that the virus spread like wildfire among US white-tail deer, and demonstrates a few more instances of spill back from the deer to humans. Not surprising given the much earlier Danish evidence of spill back from farmed mink to humans. The virus is not only a permanent feature in humans going forward, but likely will remain in various animal reservoirs, undergoing continuous mutation and perhaps spilling back with unpleasant results. A group from Washington University has just reported on a device which measures COVID virus RNA in the air in real time, with a very impressive lower level of detection, and gives a signal within minutes of minute concentrations of the virus introduced into the room air. This could probably be rapidly scaled, made affordable and adapted to detect a number of other respiratory viruses—but we would have to deal with the possibility of some people screaming and running for the exits when the light on the box turns red.
Real-time environmental surveillance of SARS-CoV-2 aerosols | Nature Communications
https://www.nature.com/articles/s41467-023-39419-z
Some of you might have noted, or been relieved, that it has been several weeks since the last installment of Clear and Present Thinking. I have been hard at work on a challenging game for mobile devices called, “Whose Bag of Coke”. If you received the Beta version and solved the puzzle by simply immediately drug testing all the players with access to the virtual secure location—that’s cheating, it’s too easy.

Thanks Jeff for sharing another informative (and entertaining) article.