Covid Does Its Winter Thing Again
STD’s get some love

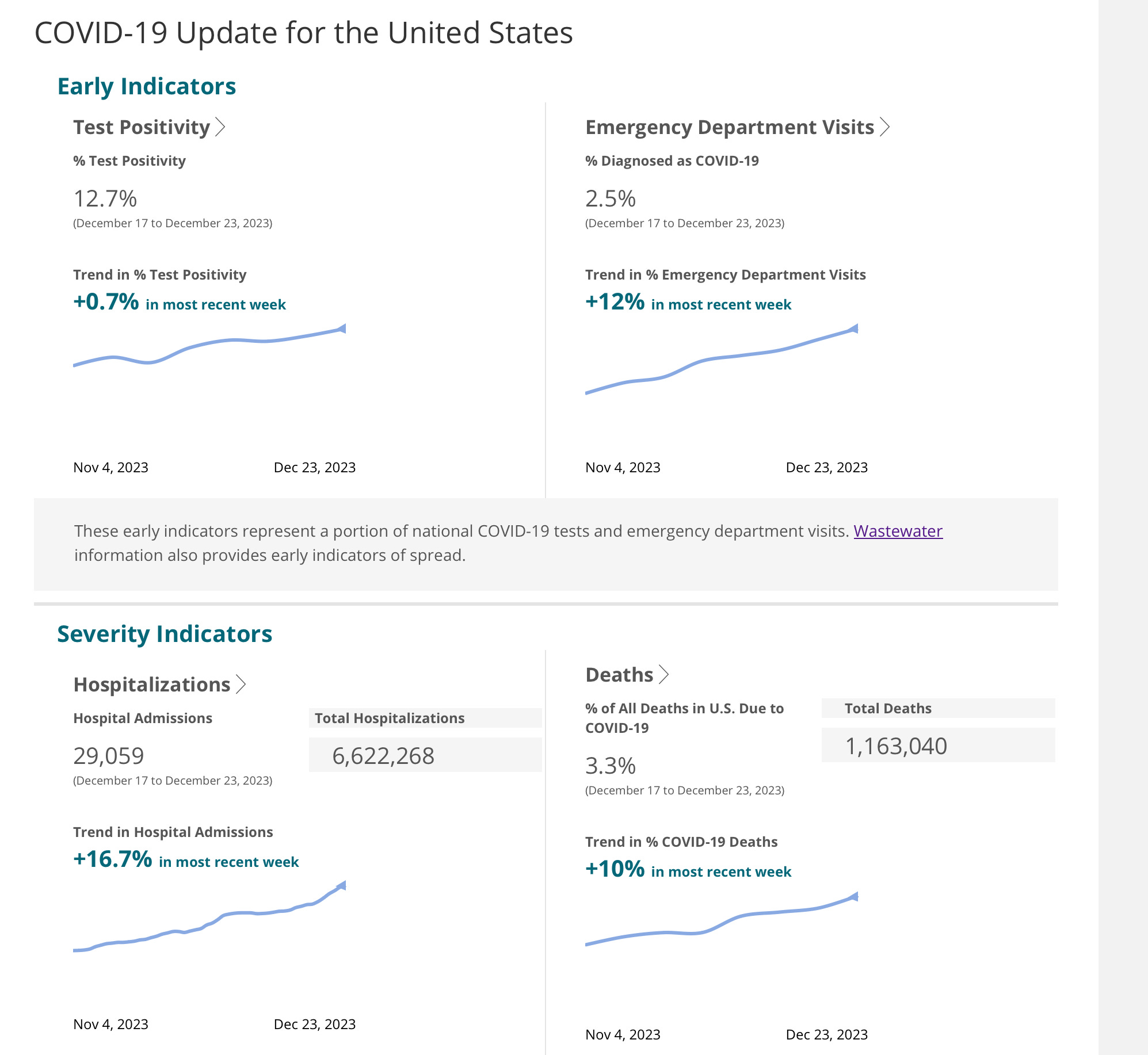
If it seems like everybody has COVID again, especially in New York, the East and West Coasts then you have been paying attention. The annual winter surge is in full swing, but hasn’t yet peaked in some western and central regions. The CDC charts here tell the tale with weekly hospitalizations about to reach 30,000, very high test positivity and rising ER visits, and of course deaths, scheduled to peak a bit later. Certainly we are doing better than prior winters—we are now 4 years into this and our immune systems have by now delighted to multiple vaccine doses and episodes of infection. The CDC won’t confirm it, but I’ve called my book-maker with a solid bet that the JN.1 variant (son of Pirola), is responsible for creating a large part of the current ramp up in cases. This variant which was 7% of COVID virus in late November is now causing 44% of infections nationwide, and higher in some areas. We haven’t seen a variant dominate like that since the original Omicron. The LA times seems content with that bet as well. Masking for staff and visitors has reappeared at several high profile hospitals, with the novel twist that it is now recommended but voluntary.
The Novids (those who have never been infected with COVID) of the world continue to intrigue me. They are a small percentage of the population, many fewer than those claiming the sobriquet; for asymptomatic infection was common from the beginning, and certainly is even more common now. The Novid status didn’t come from being “careful”—no matter how much you prided yourself on following the rules, four years into the Pandemic everyone has been exposed multiple times. Their immunologic amour appears to have been the elite production of unique antibodies in response to the old routine endemic corona cold viruses HKU1 and OC43, antibodies which cross reacted with SARS2-Cov19 sufficiently enough to prevent infection. Did these people also have unusually high antibody production in the nasal mucosa and upper airway? A good question that should be answerable. Then there are people who got infected, but their innate immune system, built around the antiviral response system linked to Interferon, immediately kicked into high gear and stopped the virus before it could cause any noticeable disease. Not true Novids, and most of these people would have mounted a telltale antibody response, which would allow us to know that the earliest stages of infection had in fact occurred. Rare people with genetic defects in this innate first defense system suffered critical or fatal disease even in the absence of the other recognized risk factors of age, obesity, and underlying severe medical problems. A recent study from China shows that a small percentage of people infected with the first round of original Wuhan virus produced antibodies which were unusually efficient in neutralizing a large number of the subsequent variants. Those would be the folks who contracted COVID only once, perhaps with or without the benefit of subsequent vaccination. You might have noticed how I refer to the original version of virus as the Wuhan strain without fear of being labeled a horrible racist. Remember how that was anathema at a certain point early on, but most of the scientific papers I read today call it exactly that. The guardians of correct-speak (or Newspeak as Orwell named it) have given us MPox, but I have to notice that this is almost always followed in the text by (monkeypox) for the edification of the non-cognoscenti, pretty much negating the correct-speak. Perhaps in a few years the monkeypox in parenthesis will disappear—but then I can foresee students, and just about anyone else asking, “Why is it called MPox, is it a myxomavirus?”

Most, of us were impressed by the breakneck speed with which effective vaccines were developed for COVID. The clinical trials of the mRNA vaccines suggested an extremely high efficacy in preventing infection. From a vaccine PR point of view it would have been smart to anticipate early on that there was a very high likelihood these vaccines would never be SO much more effective than any respiratory virus vaccine ever developed previously. It would have been smart to concentrate early messaging on the reduction in disease severity offered by vaccination, rather than have to continuously lower the bar on their effectiveness in preventing infection. As you can see I am extremely gifted with hindsight, but there is an important lesson for the future here. To put into perspective just how difficult vaccine development can be, consider that the only ongoing large scale HIV vaccine trial has just ended in failure once again. That is despite 40 plus years of modern medical science, with the greatest investment of money and resources ever committed to developing a vaccine. RSV might have come across your horizon for the first time last year with the approval of the 2 new vaccines, but it has taken 30 years of active vaccine development to achieve this. With public confidence in vaccines steadily declining, against a backdrop of social media disinformation and mal-information, it is extremely important for the scientific community, public health and government to disseminate information which is not only scientifically accurate without political spin, but anticipatory of objections and lines of attack from the non-scientific, highly skeptical community. The worst mistakes are: first to ignore signs that efficacy in the real world is falling well below heavily advertised clinical trial results; second to pretend that uncommon side effects, which the clinical trials were never powered to detect, are “exceedingly, impossibly rare”, before you have real data to address the actual frequency. Another massive mistaken in my view was to mandate vaccination of low risk individuals after it had become clear that the vaccine did not efficiently prevent infection and forward passage. Nothing breeds suspicion and resentment more than coercion, especially when it is manifestly apparent that the logic is false and the narrative untrue. Times have changed from the pre-social media era when most folks would willingly line up to take whatever was being ordered by the government. You can’t play catch-up or do-over in the court of public opinion regarding vaccines, there is too much venom and mistrust. While the US hit a home run with best COVID vaccines, the subsequent failures were at least partially avoidable, and every effort must be made to prevent them in the future. I have never been impressed by scientists or public figures who purport to be concerned about uptake of vaccines, but offer either overt or thinly veiled denigration of the intelligence of the skeptical. In my experience that approach has never convinced a single person to take a vaccine, and if you’re goal is truly to convince people to take a shot, and not simply trumpeting your intelligence, virtue and training—then as my grandfather used to say, “You catch more flies with honey than vinegar”.
Let’s turn now to everyone’s favorite subject, STDs (ok there might be a few people who prefer Macroeconomics, Northern European Renaissance Art History, or Numismatics but these are outliers). STD frequency has been dramatically increasing in the US over the last few years. Syphilis cases have been skyrocketing, and worst of all cases of congenital syphilis have increased ten times from 2012 to 2022! Congenital syphilis (CS) is potentially devastating to the child, and the CDC reports that last year 3700 babies were born in the US with this infection. A study from Brazil a few years ago looked at all cause 5 year mortality in children born with CS and found it was 7.8/1000 patient years compared to 2.9/1000 patient years for children without CS. That doesn’t take into account the fact that many pregnancies complicated by syphilis end in spontaneous abortion or stillbirth, and that survivors can have severe life-long complications. For women who were untreated during pregnancy, and for babies born with signs and symptoms of CS, the relative 5 year mortality rates were 2.8 and 7.1 times higher than uninfected babies. The CDC further reports that MORE THAN HALF the US cases of congenital syphilis are occurring in women who had a positive test for syphilis during pregnancy, but did not receive any or adequate timely treatment. Blame it on whatever your favorite usual suspects happen to be, but it is clear there is opportunity to do better, and we need a well thought out plan implemented to correct this.
5 Year Mortality Rates For Children Born With Congenital Syphilis In Brazil, A National Study/
https://doi.org/10.1371%2Fjournal.pmed.1004209
Us Syphilis Cases in Newborns Continue to Increase: A 10 Times Increase Over a Decade. CDC Newsroom Nov. 7, 2023.
How about the other diseases that might involve some fun in being exposed to, but no fun to acquire? Chlamydia, Syphilis and Gonorrhea have all been increasing at alarming rates in the US and many areas around the world. A strategy of using prophylactic Doxycycline post sexual encounter showed very substantial reductions in Chlamydia and Syphilis in 2 US studies of MSM (men having sex with men) and transgender women. A similar study from France, IPERGAY, showed similar reductions of 70% for Chlamydia and Syphilis. The story for Gonorrhea was different however; the US trials demonstrated a more modest reduction for this STI in the range of 50%, and no reduction at all in the French trial. This difference has been attributed to the higher incidence of Doxycycline resistance in France. On the basis of these studies prophylactic post exposure Doxycycline is now recommended for this population. My guess is that we will soon see wide spread resistance and loss of Doxycycline as an effective therapeutic—certainly for GC and likely for Chlamydia and perhaps Syphilis.
`
Most of the editorial department are out on sick leave with COVID and the 2 who accompanied President Biden on vacation returned from the Virgin Islands horrifically sunburned, and with Listeria from some unpasteurized local ice-cream. This week we had the resignation of Claudine Gay, and the flight logs of the private jet to Epstein Island (or as the locals refer to it Billy Land) made public. Will the campus culture of Harvard be materially different without President Gay, or Penn’s different without their former President Liz Magill? It’s almost a certainty the answer will be no. Gay wasn’t forced to resign because she was anti-Semitic, after all Harvard was circling the wagons to protect her on that score. She was forced to step down because she was their mouthpiece and champion of Woke/DEI ideology, and she inadvertently shined a light on the racism, intolerance and immoral nastiness of the system which has devoured Harvard. It wasn’t her fault, she couldn’t provide a decent answer to the straight forward questions posed to her in Congress, because there is no fundamental decency in the system which elevated her, and which she was there to defend. That of course and the money (always the money), the reported billion dollars in pledges which horrified alums threatened to rescind. And let’s not forget the students Harvard might try and expel for plagiarism in the future—juries in America are fond of returning jackpot awards when the defendant is perceived to have deep pockets or to make an example of them, and where are there deeper pockets than Harvard? The only material change I can foresee is that these Universities may be forced into pretending they are actually what Claudine Gay claimed, defenders of free speech no matter how racist, violent, slightly right of center or utterly appalling it might be. That should at least be amusing to watch.
If you appreciate the information and analysis of these pages then please share them.