

Deja Vu All Over Again

It seemed this week that the US media all woke up with a burning need to get the story out on BA.4/.5. The CDC and White House COVID Task Force joined in with a well publicized press conference alerting everyone to the massive wave of new COVID infections sweeping the country, but reassuring us that they have been tracking it carefully, and have everything well in hand. (I’m dropping the COVID-19 designation from here on as that seems passé in the permanent COVID era) Aggregate waste water data from around the country reveals that all of the large national regions are showing a rise now from the plateau we had been at for sometime. That includes the New York/Northeast region, where a steady decline after the wave of BA.2 and BA.2.12.1, which they experienced before the rest of the country, has been reversed by the newest disease surge of BA.4/.5. The current situation is similar to what we experienced while just beginning to apprehend the arrival of BA.2, causing the second Omicron wave, and were alerted to the even more contagious BA.2.12.1. BA.4/.5 is ramping up now; and it’s deja vu all over again with BA.2.75, the latest item on the menu from India, nipping at its heels. This newest variant has been reported from at least 10 US states in the last few days, but it will take a few weeks to see how it competes against BA.5. Hopefully the BA.5 wave will provide a boost in immunity that may attenuate the spread of this newer descendant of Omicron; otherwise, we may be looking at a fall wave timed to intersect with the start of school and cooler indoor weather. I’m starting a survey here to see how many people think that BA.4/.5 will be the variant of concern circulating around by late October or November, when the newly formulated booster vaccine targeting it, which the CDC requested, will start to get rolled out. Leave your comments below.
The COVID death rate is very slowly trending upwards, and unfortunately it looks like BA.5 will push this substantially higher, just through sheer numbers of infections; similar to the experience with the “milder Omicron”. As I have noted several times before, your best protection against severe disease and death if you are older is a third dose of RNA vaccine — and of course early treatment with Paxlovid if you do get infected. Given that fact, I was surprised to hear Ashish Jha, White House COVID Coordinator, state at this weeks press conference that, “If you are at least 5 months out from your primary series, you should get a booster.” I checked with the CDC official page on booster recommendations, and that in fact is what it still says. It also says that if you are 4 months out from your first booster you may be eligible for a second booster. Beyond not making much sense up front with the difference in timing between first and second boosters, one has to wonder why they are perseverating in these eligibility criteria. The data which was used to formulate this recommendation for timing of the first booster dates from the early recognition of breakthrough infections with variants, and the analysis of neutralizing antibody decline kinetics, allowing for breakthrough infections even with original Wuhan. We have known for some time now that the immune evasion potential of the Omicron lineage is so powerful that the 2 shot primary vaccination series does not provide adequate protection form severe disease, and that a third jab greatly enhances this protection. Will anything bad happen to you if you take the third shot sooner than 5 months? Certainly not, and given the huge number of at risk, un-boosted individuals, I can’t imagine why the CDC is persisting in this outdated scheme. Lives could be saved by getting, especially older, people boosted; and in my opinion no one should be waiting now for 5 months to elapse before taking a first booster.
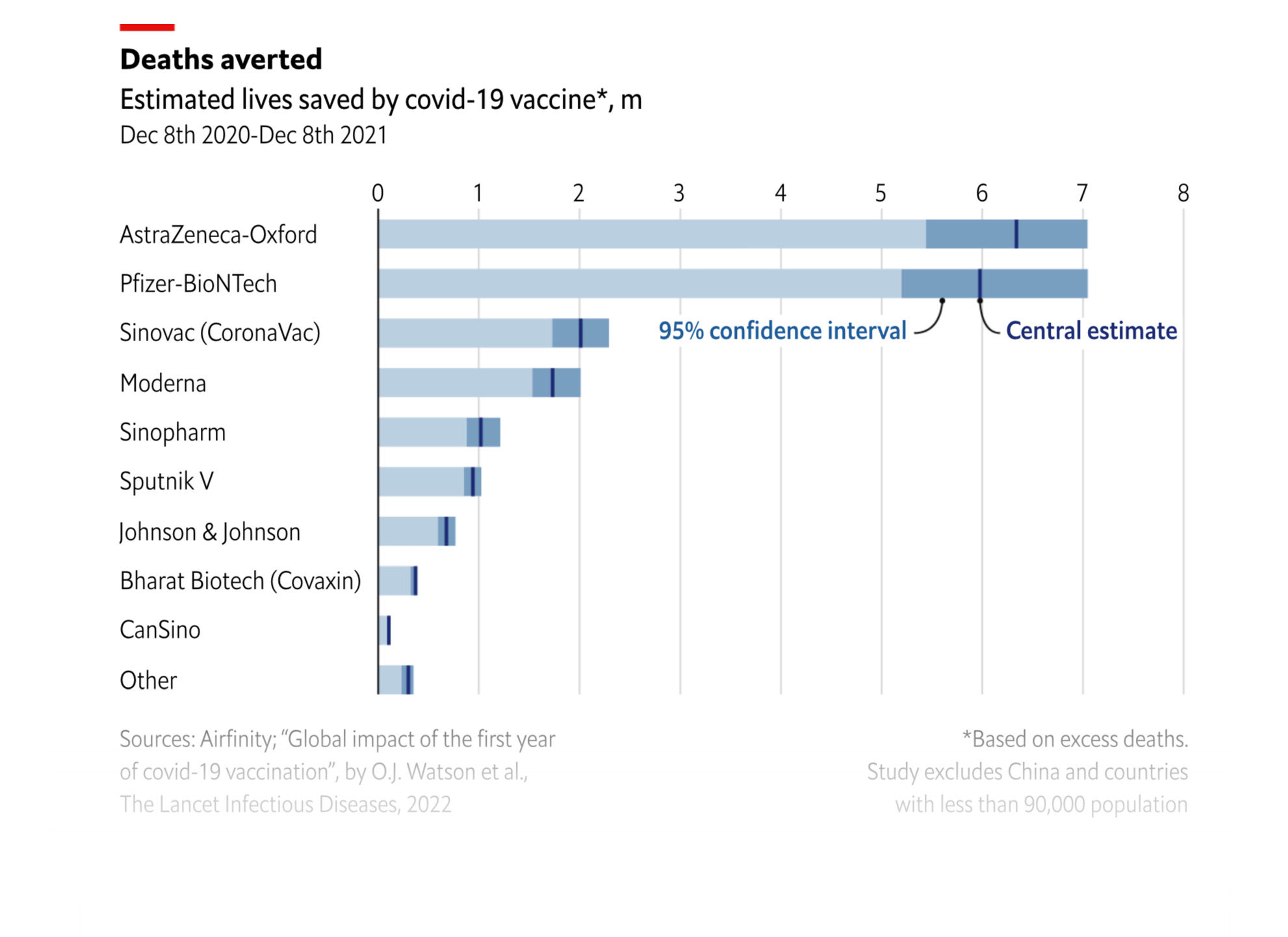
Recently we learned that the best estimate so far is that the vaccines saved at least 20 million lives around the world in 2020. Here is a nice graphic taken from the Lancet study by O.J. Watson which details the relative contributions of each vaccine if you want to cheer for your favorite. (Some less effective versions make the list simply by the huge number of recipients.)
I have been asked repeatedly about my opinion on second boosters, and I will try to efficiently summarize here. The data on a reduction in the risk of severe COVID following a fourth dose of vaccine came first from an Israeli study published in the NEJM in May. This was a large cohort of people over 60 yo and the reduction in severe disease during the four weeks following vaccination was in the range of 2.5-3.5 fold. Reduction in infection was 2 fold, but began fading by the end of 4 weeks. Similar data has just been published by the CDC in the July 15th MMWR for an American cohort, and it’s worth giving an overview of that. During the BA.1 Omicron period, the third dose of vaccine, 120 days post dose, provided a VE (vaccine efficacy) against hospitalization of 85%, but that similar time frame efficacy was down to 52% during the BA.2 and BA.2.12.1 period, due to further immune escape. This is efficacy compared to unvaccinated people. The critical data during the BA.2 time frame showed that VE was increased from 55% to 80% by a second booster, but the average duration of time from the fourth shot was only 27 days. If you persist far enough into the MMWR paper you will see that the VE of a second booster declined to 26% at 120 days post the dose. Both studies are referenced below.
N Engl J Med 2022; 386:1712-1720 (Israeli study)
DOI: 10.1056/NEJMoa2201570
http://dx.doi.org/10.15585/mmwr.mm7129e1 (MMWR July 15)
This data was all generated during the earlier Omicron wave when BA.1 and BA.2 were the circulating viruses. BA.4/.5 is now the dominant virus and will very soon be essentially the only virus. It has substantially greater escape from the neutralizing effect of vaccine generated serum. A study from Harvard in this weeks NEJM details this for anyone interested.
“Neutralization Escape by SARS-CoV-2 Omicron Subvariants BA.2.12.1, BA.4, and BA.5” http://dx.doi.org/10.15585/mmwr.mm7129e1 (MMWR July15)
So in summary: a second booster induced a measurable increase in protection from hospitalization against BA.2 that was short lived. My guess is that the marginal reduction in severe disease offered by the second booster dose has likely been circumvented by the wily BA.5, but that is just conjecture. If you are over 50, or otherwise eligible for the second booster, I advise going with the only epidemiological data we have available. If you were boosted once but subsequently had infection since January (the Omicron lineage era), I would hold off, the evidence is pretty clear your immunity now is at least equal to, and probably better than double boosted folks. There are theoretical reasons to avoid repeatedly challenging your immune system with a vaccine designed for a now extinct virus, and we should carefully weigh the balance of risk and reward.
I’d like to touch on the topic of long COVID, which I know is on many people’s minds as they take stock of their risk tolerance and plan their lives. The quick and accurate answer is that nobody really knows what the risk is, and various published studies have delivered results similar to the proverbial Monkey throwing darts. This is not unexpected when the syndrome being studied is poorly defined, and even more poorly understood. My conviction is that Long COVID falls into a number of categories that are difficult to separate clinically. There is “damage done”, generally the result of the more severe cases; and the consequence of massive organ insults, multiple small strokes, myocardial damage, multiple vascular occlusions in the lungs and decreased diffusion capacity, kidney damage and others. When you are hit by a bus, the orthopedist may put your shattered leg back together, but your chances in the 220 are now gone. Then there is a category of post COVID symptoms that appear likely to be caused by delayed clearance of the virus, and persistence of viral antigens which cause continued immune system reactivity and inflammation. There is a growing body of literature detailing this phenomena in the CNS and in the GI track. There are also certainly people with previously undiagnosed or preclinical mental illness which is unmasked by the stress of illness and isolation, and many of their symptoms may be purely somatic. Then there are the malingerers who will try to take advantage of whatever freebies are eventually floating around. There are opinions, and some studies, to suggest that every episode of COVID gives additive risk of a long term syndrome. It doesn’t take much of a leap of faith to credit studies which have concluded that higher risk is associated statistically with more severe disease. A meta analysis of many published studies from around the world came to the conclusion that prolonged symptoms may be occurring in about 2-3% of people who experience relatively mild disease. Since nobody really knows, I have to fall back on, “You pays your money and you takes your chance”.
Finally Tanzania is making the news with reports of a dozen people from a single village with a so far unidentified disease causing fever, myalgias, prostration, headaches and nasal bleeding. Oh, and a 25% mortality so far among the identified cases. Sure sounds like a hemorrhagic fever virus, but tests for Ebola and Marburg are negative. It’s the wrong part of Africa for Lassa fever, which has a far lower mortality rate. Other possibilities I suppose would include Rift Valley fever (also a lower mortality rate) Crimean-Congo hemorrhagic fever, Lujo or some novel, never before seen virus. Updates will certainly follow on this, but it’s a safe bet to say we all may have a heightened interest in unusual diseases in distant lands for quite some time.
We are all feeling our way around a new adjusted reality, where the healthy and young are at little risk of fatal disease, but cognizant of the possibility of a nasty brief illness and all the inconvenience that entails. For the older group which includes me, and those with serious underlying medical issues, the words of a famous detective sum it up, “Are you feeling lucky today punk— well are you?”
Thanks once again for your time, and for your referrals of this page to other readers.
Just an opinion. Most of the patients we are seeing at this juncture for elective procedures might as well be considered unvaccinated, they not only have never received a booster, the only series received was when the vaccine was first available. If the vaccine is to be considered as effective as flu vaccine then a majority have no protection. NJ no longer requires testing before an elective procedure “ if the patient was vaccinated “. Basically we are left to just assume everyone has Covid, as we did in the days of early AIDS, best practice everyone has it take appropriate precautions. Quietly they’re urging people to wear masks again, but most will not, having had recent Covid myself it wasn’t the run of the mill cold, I will avoid reinfection at all costs. Sadly, I suspect we’re chasing our tail.