Harvard is Trampling the Truth
Plagiarism is fun and easy

Since plagiarism seems to be all the rage for certain academics at some elite universities these days, (not to mention politicians) I thought I would plagiarize the title of Martin Kulldorff’s article in City Journal. For those of you not familiar with ex-Professor Kulldorff, he was a highly respected epidemiologist and Professor at Harvard—that is until he dared to publicly question the early, pre-vaccine lockdown policies of our government, the CDC, Anthony Fauci and many others. He was one of the three authors of the Great Barrington Declaration in the late summer of 2020, and his current article details the program of castigation, cancellation, insults and innuendo; which was orchestrated by: certain academics embracing the prolonged lockdown approach, the media, NIH, CDC, and culminating in his firing from a tenured position at Harvard. If you are not familiar with the Great Barrington Declaration—even if you are, it has been more than three long miserable years since you first encountered it—and it is worth a quick short read now with the benefit of hindsight into how the Pandemic ultimately played out. Remember for context that these ideas were written before there was a vaccine available, and before it became obvious that SARS2 would become the shape shifter and antibody escape Houdini that it is.
Sweden was the model for an advanced liberal country which pursued a program of pandemic response concentrating on protecting the truly vulnerable, while allowing society to function as normally as possible—with the understanding that infection acquired protection from severe disease was a real thing, just as it has been throughout the recorded history for human plagues. Real protection for people at high risk from respiratory communicable disease can only come through enough of the population acquiring immunity (either by infection or vaccination) to dramatically decrease transmission of the disease, unfortunately named “herd immunity”. Sweden was virulently criticized by the same mob that attacked Kulldorf and the other authors of Great Barrington. Now almost four years later, we know that Sweden ended up in the middle of the pack for early COVID deaths among western European nations, many of which adopted the draconian lockdown approach. More importantly, over the subsequent years Sweden has had the lowest excess mortality rate of any of those European nations. That excess mortality rate, which I discussed in prior blog installments, includes not only direct COVID deaths but captures all the excess deaths which were a result of the incredible disruptions of normal social functioning—the deaths from lack of follow-up medical care, treatment and screening, drug addiction and overdose, depression and suicide, and in the case of poorer nations, deaths from extreme poverty when richer nations economies collapsed and they stopped purchasing the goods which are the backbone of those third world economies. To that list of excess mortalities I would add the much discussed and devastating loss of education, never to be recouped by the poorer members of our society, and one more thing—as Steve Jobs liked to say. The lockdowns of society triggered a severe recession and massive unemployment. To combat that the Trump and Biden administrations pumped trillions of newly printed dollars into the economy—the result of that is the persistent inflation bedeviling the country. While not measurable in mortalities directly, it is a source of considerable misery; not for the wealthy and elites of society, who were generally content to go along with the program of shutting down commerce, but again for the folks on the lower rungs of the social ladder. Since it is Federal budget season our elected leaders, starting with the President, but unfortunately many members of both parties in Congress will of course now argue to print trillions more, in the time honored practice of buying votes—and then pretend they don’t understand how inflation is happening.
My intent is not to defend the Great Barrington Declaration using the convenience of hindsight to appear smart. Whether you are convinced that the authors of Great Barrington were prescient or not is really immaterial, for future histories and scientific analysis will decide that—the bigger story is the extreme nature of the response from many in the academic, scientific and public health realms. (I like that word extreme and how its meaning has recently changed. When you look it up in the dictionary it is not defined as, “Someone who disagrees with you, and presents logical arguments which can be debated”). The rabid intolerance for opposing points of view has infected our universities, government, media, and some members of the scientific community. That is to the great detriment of scientific discovery, and the trust and appreciation of science among lay people. Today’s “Scientific Truth”, may be soon in the dust bin; what is important is that the process of getting ever closer to the Truth remains inviolate, and attacking, shaming, dis-crediting and silencing informed minority opinions threatens that process at a fundamental level.
Two installments ago I discussed the safety of the food chain and how both intentional and unintentional lead contamination poisons people around the world. Today I’d like to draw your attention to the issue of how dangerous and poorly understood the vast array of chemicals contained in plastics is. A recent article in Scientific American describes the just released findings of the PlastChem Project, by a group of scientists in Switzerland and Norway which has for the first time produced a comprehensive database of more than 16,000 chemical found in various plastics. These scientist categorize about 25% of these chemicals as of significant concern for being either: “forever chemicals”, which do not readily degrade in the environment, having the ability to steadily build up over time in the human and animal bodies, mobility throughout the environment, or known toxicity. 10,000 of the chemicals they list have either no or extremely limited information available about potential toxicity and long term health risks. These plastics are ubiquitous, and if you think you can avoid them by not drinking beverages in plastic bottles, you are mistaken as they are present in floor and wall coverings, clothing and mattresses, melamine dishes and utensils, car components, and just about everything we touch. Some of the chemicals with known health consequences, which are endocrine disruptors or carcinogens, include: phthalates, bisphenols, PFAS, and a variety of flame retardants. Living in a high altitude ski town I was surprised to learn that some of the PFAS in our drinking water may have come from ski wax, where they were used for years. Below is a link to the article—and while we are at it let’s take a look at a graph of which countries dump the most thousands of tons of plastic into the oceans every year.

Does any of this play a role in the rapidly rising rates of early onset cancers affecting younger people around the world? You might be aware of the increasing numbers of colorectal cancers affecting Americans under the age of 50, but the problem is world wide with recent evidence showing the early onset incidence rates of more than a dozen different cancers is increasing at an alarming rate. With so many different diseases being involved the causes must be multi-factorial; but 16,000 plastics chemical being dumped into the environment, 4000 of them felt to be potential serious health risks and the bulk of the rest essentially unknowns, that should not give us a warm and fuzzy feeling.
For those of you who expect the COVID data update, it is here as usual. The CDC graphs following show the now rapid recession of the winter surge with significant declines in COVID emergency room visits, deaths down nicely, and “only” 15,000 folks hospitalized for the virus last week.
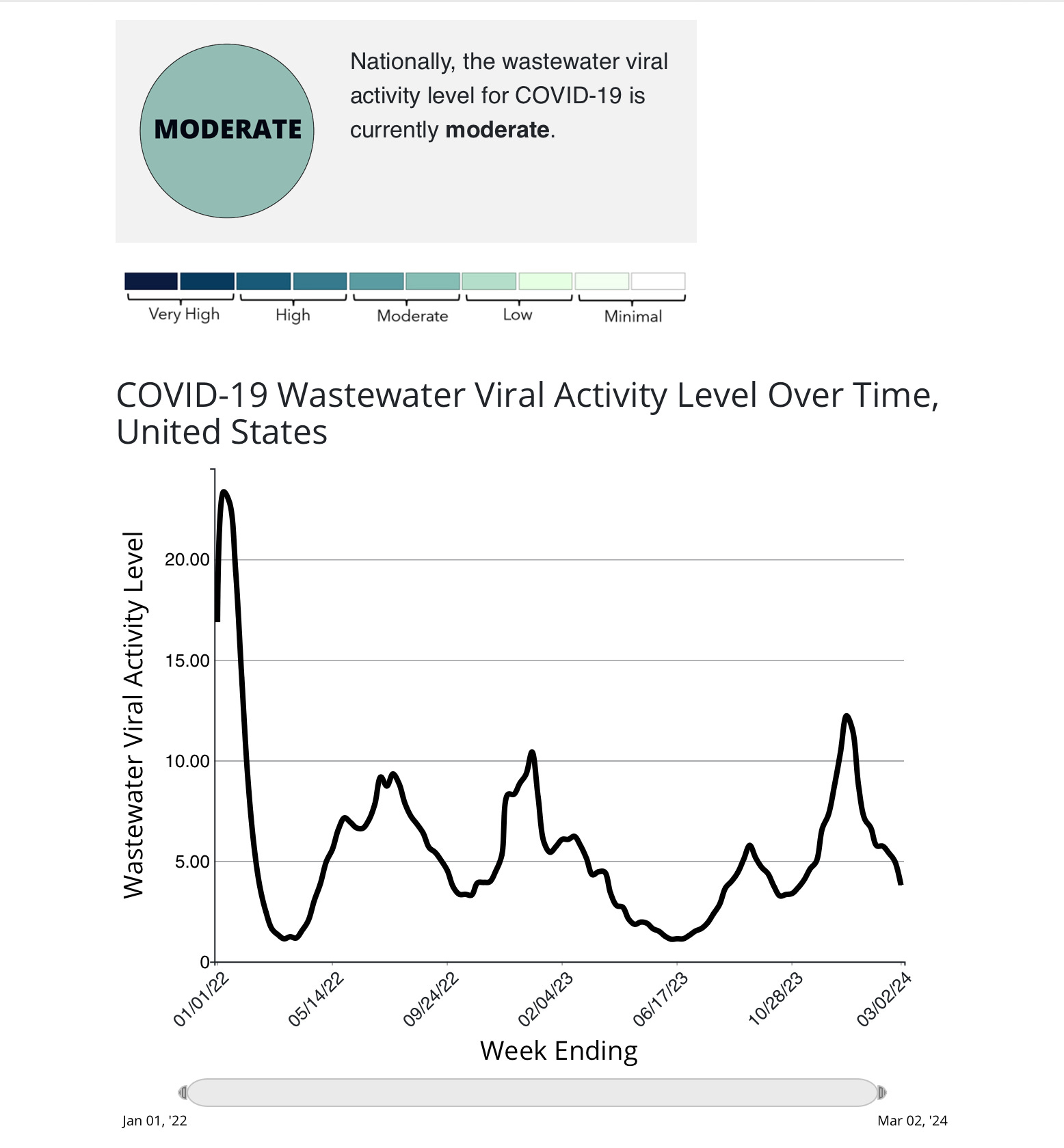
I will show you another graph of the measurement of SAR2 viral RNA in the nation’s wastewater over several years, it illustrates the scientific dictum, “the poop don’t lie”. Notice that there was more virus circulating this winter than at any other time since the original Omicron wave in the winter of 2022—so much for the initial fantasy that we would eliminate the virus through vaccination and post infection immunity! Earlier in the Pandemic the waste water SARS2 levels correlated more closely with the clinical disease burden of cases, hospitalizations and deaths. That has changed for three simple reasons: first, we are doing only a tiny fraction of the clinical testing which was done even a year ago, so mildly symptomatic cases are not identified, second, four years into the Pandemic the population has built up sufficient immunity so that the vast majority are protected from critical disease. The third reason is the unhappy fact that huge numbers of the most vulnerable have been killed off already. The second and third facts add up to an apparent lessening in the virulence of this virus, which none-the-less continues to infect us at near record levels. It is impossible to know how the current JN.1 variant would stack up in terms of virulence against the original Wuhan strain, because there is no remaining naive population.
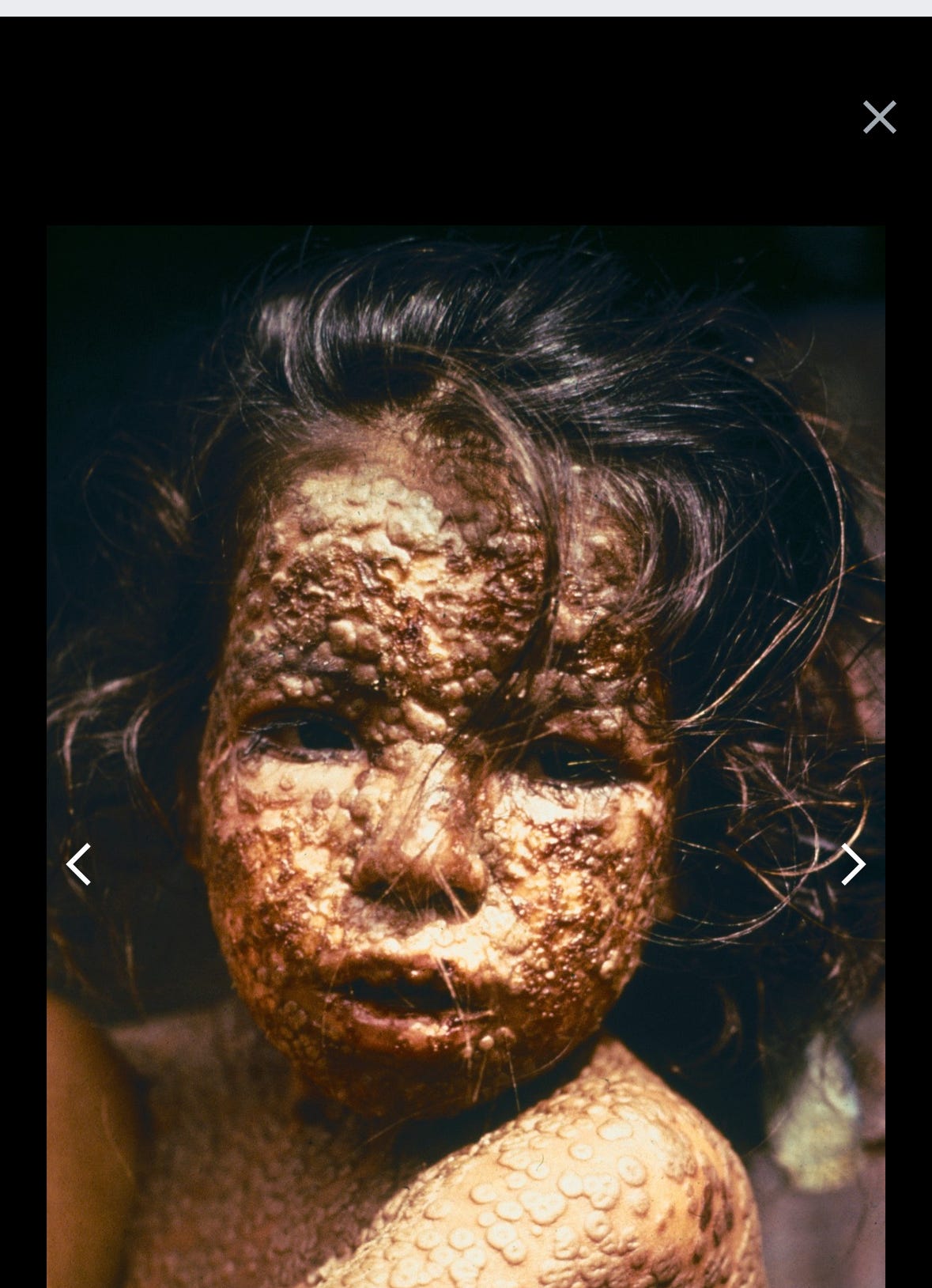
What about Smallpox, you might ask, after all we did get rid of that scourge. True, but it took 200 years from Jenner’s first successful experiments using Cowpox inoculation until the last human case in 1977. We had a chance with Smallpox virus for a variety of reasons: it is a DNA virus not prone to rapid mutation; it is not an airborne pathogen, and infection generally requires close prolonged face to face contact or direct fomite contact; almost all cases are symptomatic making contact tracing and isolation feasible; and survived infection confers life long complete immunity. None of those characteristics are shared with SARS2. While we are discussing Smallpox it’s worthwhile noting this was no light weight virus, having a mortality rate of 30% (50% in babies) compared to the SARS2 world wide mortality of <1% (actually closer to .1% using a figure of 7 million deaths/8 billion people) with infection having occurred in the vast majority of us. Also, Smallpox survivors were left scarred and sometimes blind for life. Only one other virus that I know of was eliminated by human action and that was Rinderpest, a severe infection of cattle and other ungulates, and a serious threat to the food security in Africa, India and the Middle East until its elimination in 2010. That was accomplished through vaccination and destruction of infected individuals—not a popular means of human infection control, except perhaps in North Korea. The following picture of a child with Smallpox might be disturbing to the non-medical folks.
With all that has been measured and written about Long COVID, I still feel we are lost in the many trees and missing the forest. The vastly different ways in which acute COVID can affect different individuals: from asymptomatic to isolated anosmia, critical pulmonary failure, life threatening blood clotting, neurologic derangements etc., is likely similar to the spectrum of disorders lumped together as Long COVID. The following article in Nature, from the UK, is interesting for their discovery that between .1% and .5% of people with acute COVID had persistent high level viral replication going on for at least 60 days. Those people had a 50% chance of reporting persistent symptoms that we would call Long COVID. Now that is something you can hang your hat on, a unique (although small) group within the Long COVID category where directed antiviral therapy may actually be helpful. On the other hand, I’m not optimistic that the Paxlovid studies for the general category of Long COVID will be positive. The other interesting finding of this study is that some of these chronically infected patients had rapid evolution of viral mutants, while others had quite stable viral sequences—that likely reflects the varying degrees of selective pressure generated by their immune response.
Prevalence of persistent SARS-CoV-2 in a large community surveillance study https://doi.org/10.1038/s41586-024-07029-4
In a final quick infectious disease update, the CDC has sent a team to Chicago to address a potentially explosive situation of a measles outbreak in a shelter for illegal aliens. As of this writing 10 cases have been identified, with 8 occurring in the shelter population. The CDC is reporting that approximately half the 1900 people in this temporary shelter, which was designed to hold 1000, were determined to be immune to measles, and almost all of the other 900 who were eligible have been vaccinated. That would suggest the vaccination rate of this population is vastly below that of the US, and further cases are expected as vaccination is only reliably effective if administered within 72 hours of exposure. The latest published CDC statistics suggest that the overall US vaccination rate for measles in children 24 months old is around 90%, and 92% in adolescents. It is likely lower than that given the recent uptick in vaccine hesitancy, and lower certainly in certain sub-populations and locales. That means we are below the threshold for preventing sustained transmission in the community and not just occasional random cases. Accompanying the CDC team was RFK Jr. providing information to the migrants about the extreme dangers of vaccination, and suggesting that they lobby the city of Chicago for bus tickets to Florida where pesky public health officials won’t harass them to get vaccinated or quarantine.
The editorial section today is on rebranding and Newspeak, skip it if cancel culture has effectively eradicated your taste for sarcasm, comedy, and generally making fun of absurdity. Rebranding has accelerated to the point where it’s difficult to keep up. Monkeypox was renamed Mpox, really a bad choice since we already knew that monkeys are not the natural reservoir of the virus—African rodents are—and everyone who looks at Mpox hears Monkeypox anyway. I am proposing further rebranding to aRpox (the first letter not capitalized so nobody is tempted imagine any relationship to Africa). African Swine Fever, Congo-Crimean Fever, Ebola, Marburg Virus, German measles and dozens more are also desperately in need of social justice rebranding. Then there is the issue of what to call people who have entered the country illegally. They were always illegal aliens (and remain so according to Federal Law) but then they became “migrants” under Newspeak. That term had a distinctly negative connotation—I can’t imagine what the folks at the Ministry of Newspeak were thinking when they let that one fly out the door. So they became “undocumented persons”. Even President Biden, who has access to the top people at the Newspeak department can’t keep up. After his State of the Union address he apologized for calling the murderer of Laken Riley an illegal alien, and admitted he should have said “undocumented person”—but Newspeak has already moved on and these folks are now “new comers”. Once again the Newspeak department blew it with “undocumented” having a less than savory appeal, suggesting deficiency. The word on the street now is that some of these people who have been here for a few years are unhappy being called “new comers”, so I am proposing a further rebranding to “Cultural Ambassadors”. My application to work for the Ministry of Newspeak will include my suggestions for other groups who have been unfairly disadvantaged by current English language usage. That would include mass murderers, who would like to be called “people experiencing anxiety about overpopulation”. People who push others onto the subway tracks will no longer chaff under the pejorative “attempted murderer”, but be “persons experiencing anxiety around trains”, and January 6th visitors to the Capital who lobby to have “insurrectionists” replaced will henceforth become “tourists lacking a current guide to Capitol visiting hours”. (Nod to Babylon; Bee on that one). Similarly folks refusing to pay their taxes because they don’t agree with certain government policies will no longer be “tax cheats”, but “conscientious objectors”. To avoid confusion, the individuals who have previously refused to serve in the armed forces because of religious or ethical beliefs will now be called something else, or perhaps just forced to serve given our dismal recruiting numbers in the last several years.
