How Do YOU Evaluate Risk?

In my last post I mentioned that the expected summer COVID wave appeared to be finally showing up, later and perhaps weaker than “usual”. CDC data through August 16th now confirms that is the case, both in terms of test positivity and ED visits. So far the Western and Southern portions of the country are experiencing the highest levels of transmission. It’s that time of year when some people will be looking to get another COVID booster, and others will be pondering whether it is really worth it. Part of that calculus is having information on how effective last year’s shot was at preventing serious disease, since we are now well into the sixth year of building both natural and vaccine immunity. A study just published in Vaccine provides some useful information, but also highlights an issue I have discussed in the past, the presentation of study results as relative risk versus absolute risk. The investigators looked at a cohort of 6,900,361 random people with commercial insurance from California and Louisiana during the fall of 2024-early 2025 time frame, and asked the question, what was the relative risk of hospitalization with a COVID diagnosis between folks who received last years Pfizer vaccine versus those that did not receive a COVID booster? (The study was supported by Pfizer (who could have guessed) and the authors report affiliations with Pfizer and other other Pharma industry interests—but I think the results are worth looking at).
Overall only 4.7% of this very large group received the Pfizer vaccine. The CDC reports that about 21% of adults over 18 years old received ANY COVID booster last year, and about 12% of children under the age of 18. The study analysis showed that overall vaccine effectiveness in preventing COVID associated hospitalization was 41%, and 45% in the group over 50 years old. That’s what is referred to as the relative risk reduction. The 95% confidence intervals were extremely wide, sort of perplexing for a study with this many participants—but I think a look at the absolute risk provides the explanation. Vaccinated people had an absolute risk for COVID hospitalization of 2.2 per 100,000 verses 4.1 per 100,000 for those not receiving a booster. Such a small fraction of the overall population is currently getting hospitalized when they acquire COVID (which they do in droves, especially in the winter) that a single person from either group randomly being hospitalized out of 100,000 will immediately skew the absolute risk data, leading to the huge confidence interval spread. There is another confounder in this retrospective observational study, which very clearly might make the booster appear more effective than it actually was. The vaccinated group had higher rates of having had an annual exam during the preceding year, plus higher rates of influenza and shingles vaccination. Isn’t it likely this group might generally be more attuned to closely monitoring their overall health, have other medical problems identified and under good control, and perhaps be more likely to contact their physician at the first sign of illness—perhaps even getting a prescription for a COVID anti-viral or other medication? We all evaluate risk differently and some might feel that time off to go get a COVID booster, and put up with side effects (if you have any), is worth reducing your risk of hospitalization by 1 or 2 out of a hundred thousand. These statistics apply only to the generally healthy since there were few immunocompromised people in the study cohort, and their risk was not specifically addressed; equally this does not apply to the elderly since the average age of the booster recipients was 55 and the non-vaccinated 45 years old. The media tends to report medical study results in relative risk percentages—they are always more dramatic, and grabbing eyes and selling copy is always the point. Let’s have a look at some other recent medical risks that have made the front page, or much more likely your favorite website.
Red meat is bad for you and causes cancer; the WHO recently informed us this long suspected fact is true. The branch of the WHO charged with researching environmental causes of cancer is the International Agency for Research in Cancer (IARC). They report the “hazard” of various things of interest and group them into categories: 1) carcinogenic to humans, 2a) probably carcinogenic, 2b) possibly carcinogenic, 3) unclassifiable, and a basically never used category, 4) non-carcinogenic. This of course tells us nothing about the magnitude of risk, either relative or absolute. There is a lot of observational data suggesting that processed red meat is more likely to be carcinogenic than unprocessed meat, and in-fact the IARC lists processed red meat as category 1, and unprocessed meat as 2a or probably cancer causing. Processed meat of course means that production has done anything to it other than cutting up the animal and presenting you with the pieces. The IARC estimates that eating 50 grams (a good serving) of processed meat every day increases your lifetime risk of colon cancer by 18%. The American Cancer Society says your lifetime risk of this cancer is 4%, so eating the carcinogenic processed red meat everyday will increase your risk from 4% to 4.72%—that suddenly seems less ominous than the headlines telling you hotdogs and bacon cause cancer. And of course unprocessed meat, which they suspect, but can’t be sure is carcinogenic, is a different animal so to speak, with an absolute risk that is certainly lower. You may not like meat, or decide not to eat it on philosophical grounds, but the majority of people probably wouldn’t make a decision to avoid something they enjoy based on a potential 0.72% lifetime risk increase.
Here is an example that supports my assessment of how most people evaluate risk. Bike riding has become steadily more popular in the US in recent years. The National Transportation Safety Board says that cyclists account for 2% of traffic fatalities, and for every billion miles traveled 30 cyclists die compared to two auto passengers. That is absolute risk, although it’s pretty hard to wrap your head around the billion miles traveled and what that means to you as an individual. Nonetheless, I don’t think many bike riders would give it up even if they knew they were 15 times more likely to die on a bike going from point A to B than in a car.

Let’s look at another popular human activity, drinking alcohol. A few months ago the IARC published a huge study looking at the results of multiple long term prospective observational studies assessing the impact of alcohol on pancreatic cancer. Alcohol is known to be a hazard for several cancers, but its relation to one of the most deadly tumors was debatable. The conclusion of analyzing all these studies was that the equivalent of two alcoholic drinks every day increased your risk of pancreatic cancer by 12%, and if you consumed the equivalent of four or more drinks a day the risk increased to 16%. The headline of a 12% increase with moderate alcohol consumption might be enough to put quite a few people off their cocktails—but what is the absolute risk? The American Cancer Society puts your lifetime risk of this tumor at 1.5% for men and 1.6% for women (anytime you live longer you get more cancers). A 12% increase on top of a lifetime 1.6% risk, takes you all the way up to 1.8% risk, or 2 extra cases out of every thousand people. I forgot to mention that they only found any positive association with this cancer for beer and spirits drinkers, not for wine—so hold the Bud Lite and pass the Chardonnay.
Alcohol intake and pancreatic cancer risk: An analysis from 30 prospective studies across Asia, Australia, Europe, and North America | PLOS Medicine https://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1004590
I previously discussed the FDA pause on the use of the Chickungunya vaccine Ixchiq in people over the age of 60. The FDA has now suspended the biologics license for the vaccine as reports of severe chickungunya-like illness among recipients have continued to grow, with a total of 21 hospitalizations, including four in the past month and three deaths attributed to the vaccine. Those numbers don’t mean anything without the denominator, but that doesn’t look good. Only 80,000 doses have been distributed around the world, and estimates of how many have actually been given are substantially lower. That would place the severe side effect rate and death rate far above what we consider acceptable for a vaccine. Chickungunya has been reported from more than 100 countries and highly variable number of travelers return to the US with the disease every year (there hasn’t been any documented transmission within the US since some cases in Florida, California, Puerto Rico and the Virgin Islands in 2019). Worldwide the mosquito is humanity’s most dangerous foe, with Putin ranking a miserable second—nets and insect repellant work fine for the skeeters, Putin apparently requires a bigger stick.

Size comparison with a penny gives a good visual of how easily these are missed.
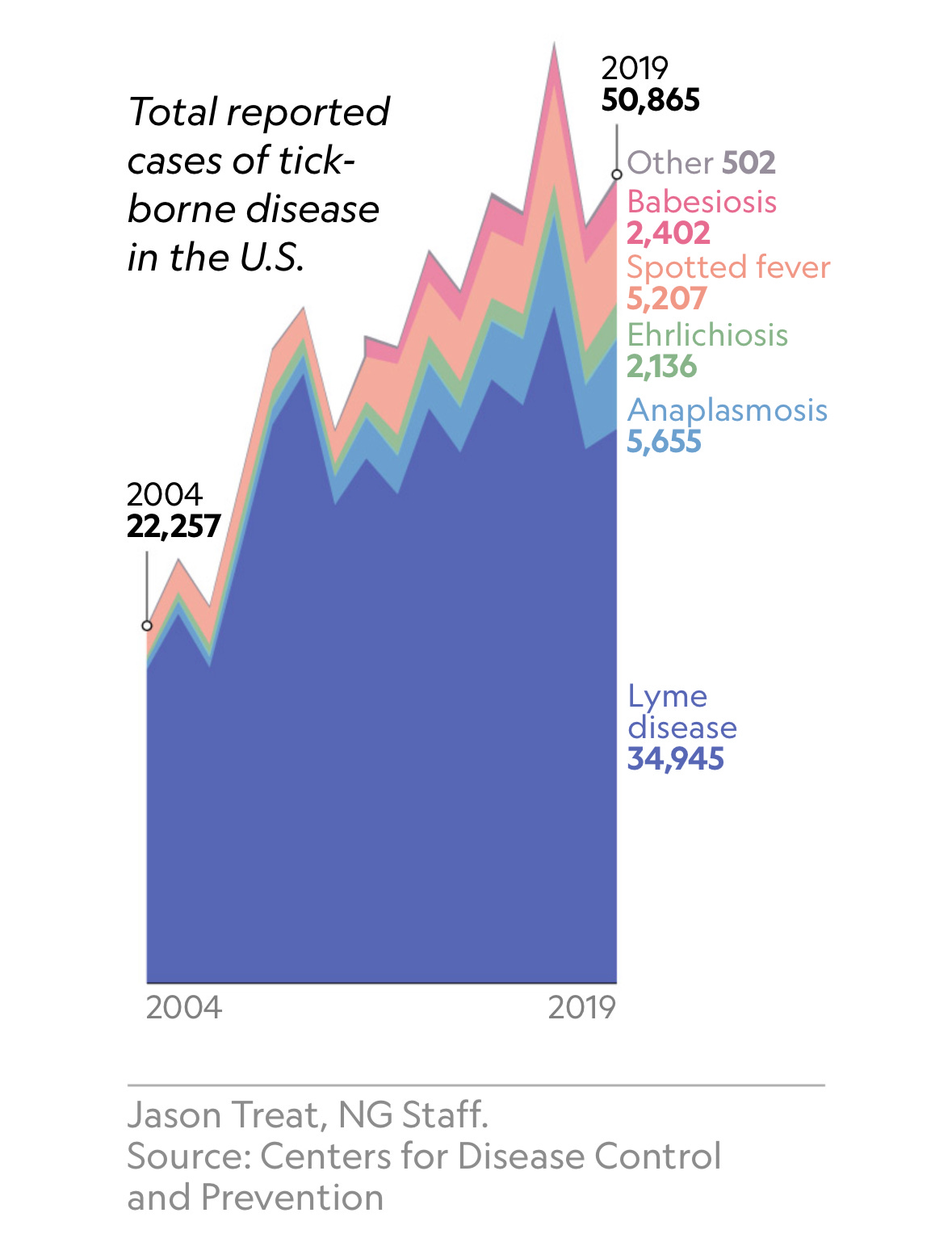
It’s prime tick season again and the incidence of tick-borne diseases has been steadily increasing with a doubling in reported cases in the fifteen years from 2004 to 2019. What fuels that increase in the most simplistic terms is an increase in encounters between people and ticks. Climate change is likely a small contributor, as some tick species populations have expanded their range northward—but other factors may be much more important. In recent years researchers have observed a steady spread of disease carrying ticks from Long Island into the more urban landscapes of Queens, Brooklyn and Staten Island, and climate change isn’t a likely explanation. Deer and the white-footed mouse are the natural reservoir for the organism of Lyme disease and its transmission to humans. In Connecticut for example, deer were very plentiful when Europeans first arrived but were nearly gone by 1900, as a result of hunting and reduction in habitat from farming. The Connecticut population of deer today is estimated to be 100,000, with humans no longer dependent on them for meat and consequently little hunting. That, coupled with steady population movement out of cities, and into suburban areas with yards, gardens, parks and golf courses in close proximity to the border of woodlands has exponentially expanded the intersection of people with ticks. As a result, more and more people will acquire tick transmitted diseases when they are bitten in locations both suburban and urban, which only a few years ago were not considered risky. If you are vigilant you might do a thorough tick check searching for the minuscule nymphs after hiking in the woods, but perhaps not after a visit to the cemetery in Brooklyn or sitting on your patio in Staten Island.
Below you will find links to two sites listing the major native tick species in the US, the human diseases each can transmit and maps showing their distribution. In addition to our collection of native ticks, the US has had an invasion of foreign ticks from around the world. This again is the result of human behavior, not climate change—ticks are quite hardy and hitch rides from all over the world on transported animals, products and sometimes humans. The most significant to date has been the Asian Longhorn tick; it first appeared in New Jersey in 2017 and since has spread through a wide swath of 21 central and eastern states, were it has become a major problem for the dairy and cattle industry. This tick transmits a parasite Theileria orientalis which attacks the red and white blood cells of cows causing anemia, weight loss and abortions. Although that parasite doesn’t infect humans, scientists have recently found Asian Longhorn ticks in Connecticut infected with the bacteria which causes the potentially severe human disease Erhlichiosis. In the laboratory it’s possible to infect this invasive tick with the agents of Lyme disease and Rocky Mountain Spotted fever, and genetic materials from B. burgdorferi, A. phagocytophilum, B. microti, and Bourbon virus (all human pathogens) have been detected in field-collected host-seeking specimens, so it seems there is the potential to have more ticks spreading these human diseases.
https://www.aphis.usda.gov/livestock-poultry-disease/cattle/ticks/asian-longhorned#:~:text=Last%20Modified:%20September%2011%2C%202024,reddish%20with%20brown%2C%20dark%20markings
J Infect Dis. 2022 Aug 26;226(3):370–373. doi: 10.1093/infdis/jiac249
The first human US case of New World Screw-worm was just reported in a traveler from El Salvador. This is the maggot of a South and Central American botfly which, unlike most maggots, invades and eats living flesh of both animals and humans. In addition to deep, even life threatening tissue destruction, secondary bacterial infections are frequent. Its scientific last name is hominivorax, which means Man Eater, and pretty much lays it out. Screw-worm flies were first detected in Florida in 2016 (climate change versus human activities?) and have caused many infections in wild mammals and some pets. Below is a picture of the worm—I’d show you a picture of the kind of human wound it can produce, but it's possible you have just eaten, and plan to sleep tonight. The second picture is of a botfly maggot of a different species that I removed from the arm of a patient who had traveled in the Peruvian Amazon more than 20 years ago. He had a large abscess like lesion on his arm which had failed to improve with several courses of antibiotics given by other doctors, and was worsening. Recognizing the breathing pore of the maggot I covered it with Vaseline and plastic wrap and waited for the worm to surface. It became a two for one medical visit when his wife passed out and collapsed as I extracted the worm from his arm.

Have a great Labor Day weekend and end of Summer season. There is already a touch of Fall in the Telluride morning air, we had to turn on the fire place in the afternoon yesterday to thaw out. As for the Culture Wars, the Cracker Barrel logo guy has been re-instated by the collapsing company, but already has job offers from multiple corporations looking to pretend they never had anything to do with the woke agenda. The most reliable rumor however is that he will be joining up with Aunt Jemima, the Land O’Lakes woman (sorry person), the Inuit boy (again sorry) from the former Eskimo Pies, and Uncle Ben to form a consulting firm advising corporate CEOs how to avoid brand suicide. Dylan Mulvaney will be creative and dance director for the new outfit. Pounding the like button at the top will insure Dylan doesn’t get cancelled again.