

Measles Runs Rampant
Important beauty tips and rejuvenation of your mouse’s immune system

My previous post discussed the measles outbreak starting at the Chicago migrant shelter on March 4. As expected this outbreak has continued to expand despite the rapid response by the CDC and local Health Department to provide mass vaccination of the shelter population. According to a measles dashboard established online by the city Health Department there were nine more cases during the last week bringing the total to 33. It appears that some residents of the shelter have come down with measles after receiving their first vaccination—not unexpected since they may have been exposed more than 72 hours before receiving vaccine. This has prompted the CDC to recommend that everyone vaccinated in the first round receive a second vaccine 28 days later, and remain in quarantine for another 21 days following the second vaccine. While there was transparency regarding the earlier cases, such as whether cases were confined to the Pilsen shelter or occurring in the surrounding community, plus various other important demographic information such as travel, prior vaccination history, etc., the city has stopped providing most data other than a daily case count and age. Almost all the early cases occurred at the shelter, but two cases have now been reported in two adjacent counties.
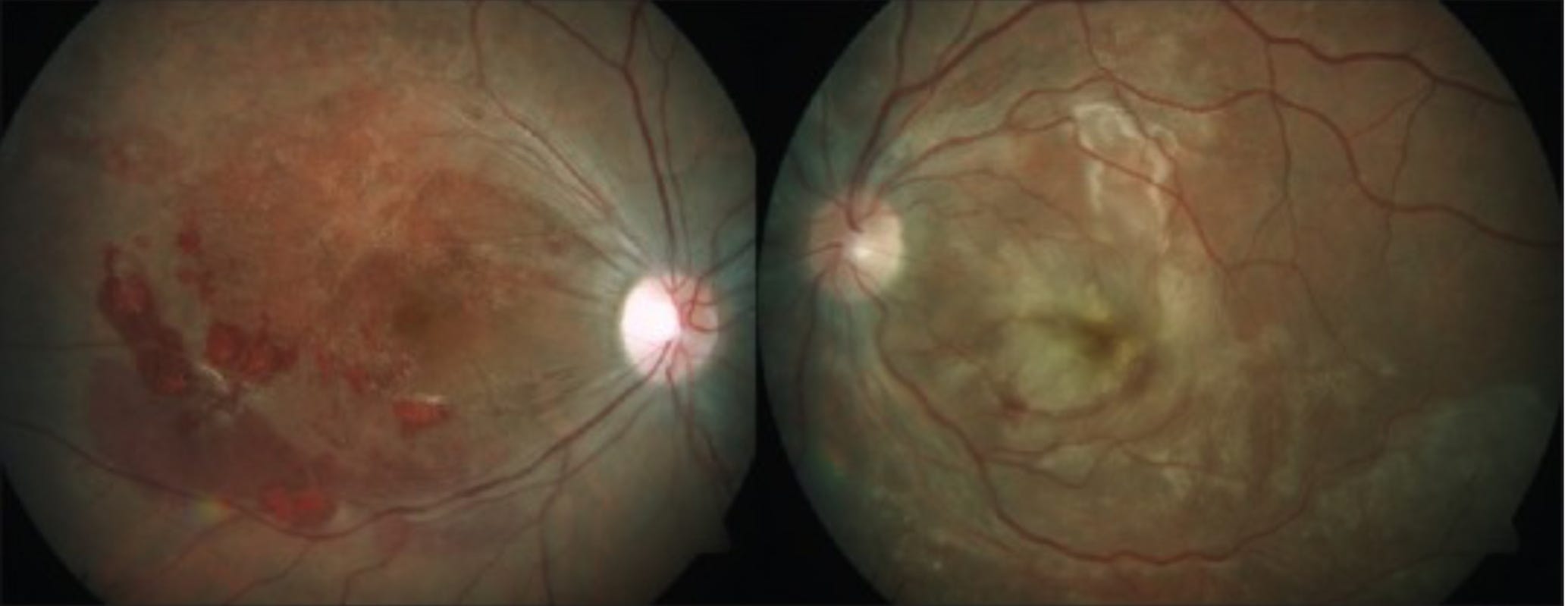
The CDC is of course strongly urging people who are not immune to get vaccinated, but it seems the language on a certain CDC web site may be causing some mild confusion. The CDC recommends that people traveling internationally make sure their measles vaccination is “up to date”. That is an interesting choice of words, and I have had two people ask me in the last week if they should get a measles “booster” before travel. Measles vaccine is one of the most effective vaccines ever developed and appears to give life long immunity after the 2 dose standard regimen in nearly everyone. Natural infection also confers life long immunity. People in the US born before 1957 are presumed to be immune even if they don’t recall infection, since the virus is so highly contagious, and was ubiquitous prior to the advent of the vaccine. If you ever had measles or 2 doses of vaccine after the age of 12 months you do not need re-vaccination. Written medical confirmation of vaccination is the standard when it comes to this serious disease, and, “I must have had it or they wouldn’t have let me into school”, falls short of the mark. If you are unsure, revaccination (assuming you don’t have a severe immune compromising illness) will be absolutely safe. Alternatively you could get a measles IgG titer done—the presence of antibodies means you are immune. Measles is exploding around the globe right now, and 17 US states are reporting current outbreaks. One in five people in the US who contract measles is hospitalized, 1 in 20 children develop pneumonia, 1 in 1000 have life threatening brain infection, which can lead to hearing loss, blindness, severe brain damage or death. Chronic measles infection of the brain in a small number of people can lead to a fatal neurologic syndrome SSPE (subacute sclerosing panencephalitis) years after recovery from the acute illness. If you like to take chances buy a lottery ticket, but don’t listen to anti-vax nonsense and fail to vaccinate your children for measles. The following picture shows measles virus infection of the retina with profound visual loss.
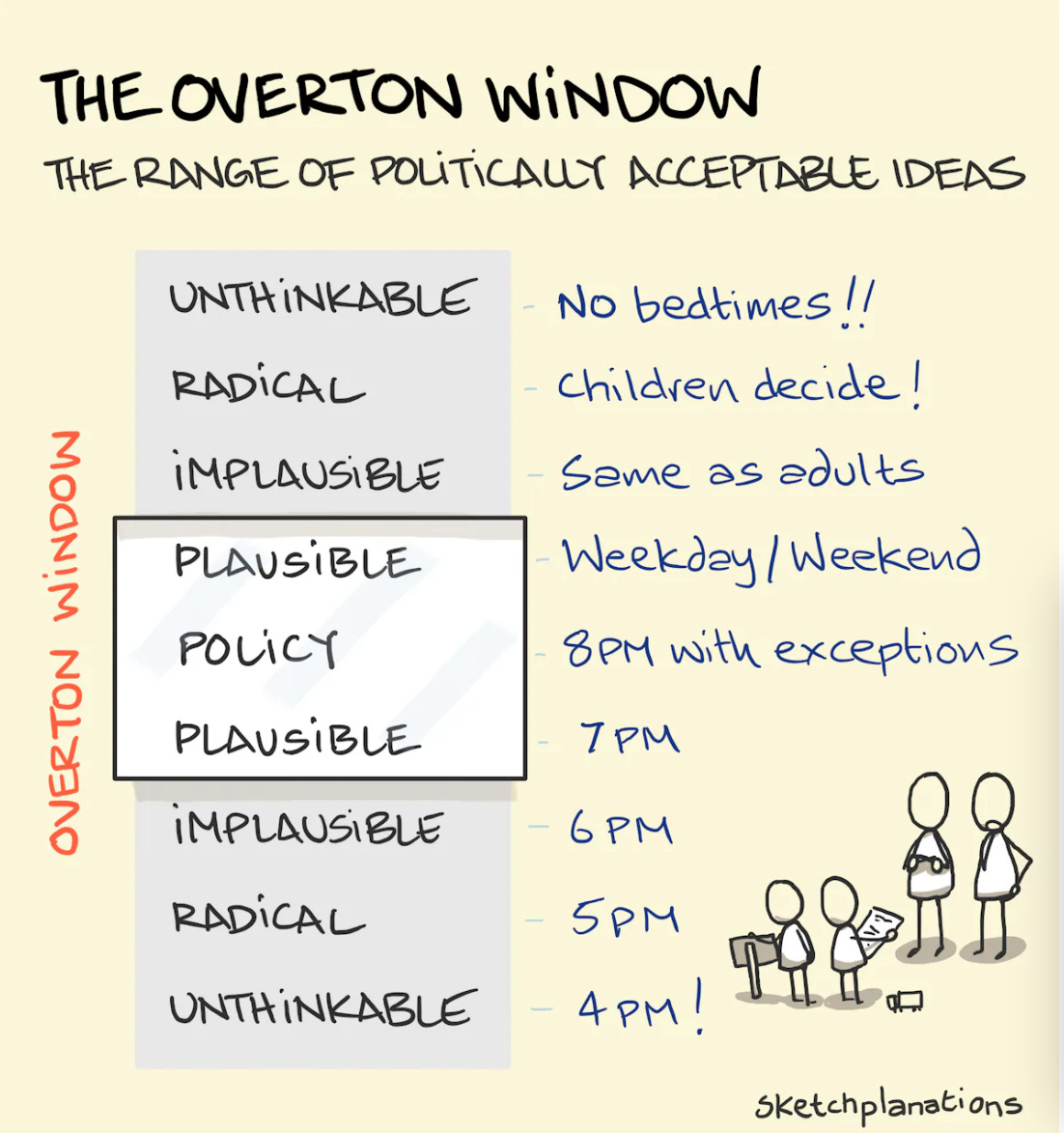
It’s officially spring; the winter respiratory season is winding down and it’s a good time to reflect on how we fared this year. Since September, influenza has caused 320,000 hospitalizations and 20,000 deaths—a very average flu year. Although most people don’t give it a second thought anymore, COVID was responsible over the same interval for double the flu related morbidity with 42,000 deaths, and hospitalizations peaking in the first week of January at 35,000/week. Starting this month, the CDC gave us new guidelines which abolished the five day quarantine; if you test positive for COVID now it’s—stay home until your symptoms are better for 24 hours and you don’t have a fever, then wear a mask when you go about your business. That’s quite a change from the days of screaming at people who wouldn’t isolate for 10 days, wore a mask incorrectly, or refused vaccination—“You are killing people”. Now I suppose it’s just less people getting killed, and the CDC realized that almost nobody was listening to them anyway. One outcome of the Pandemic may be a realization in the Public Health sector that the concept of the Overton Window is very applicable. Public Health policy has to take into account what the particular ethos of the population will tolerate at any given time and set of circumstances. Recommendations are one thing; but trying to mandate rules which won’t be followed by a significant proportion of the population, will be ineffective, lead to divineness, and disdain for the authorities.
Although only 14 % of the US population sought out vaccination with the new COVID vaccine this past fall and winter, there remains a large group of folks with severe immune-compromise who are eager for protection but fail to mount an adequate response to the vaccine. They are among the 42,000 Americans who have succumbed to the virus this winter, and have been without another option for prevention since Evusheld (a combination of 2 monoclonal antibodies) was withdrawn from the market. The emergence of newer Omicron variants in late 2022 had rendered that medication ineffective. The FDA has just approved the emergency use authorization of a new monoclonal antibody Pemgarda (pemivibart) for prevention of symptomatic disease in these immunocompromised people. Efficacy was assessed by immunobridging data, showing that neutralizing antibody titers after Pemgarda infusion are sufficient to prevent symptomatic disease from the JN.1 COVID variant, which remains greater than 95% of circulating virus. That’s great news for these people, but of course optimism needs to be tempered by the historical perspective, of how long it will be before JN.1 is replaced by the next top dog COVID, and whether Pemgarda will then still be effective. Monoclonal antibodies were life saving therapeutics early in the Pandemic, but faded in importance once the impossibility of chasing the rapidly evolving COVID adversary became clear.
I started writing “Clear and Present Thinking” as a public service during the Pandemic, and continuing in the same vein I next discuss risks associated with Vampire Facials. (I had to look it up to see if that’s a band). This is a procedure where blood is taken from the client and separated into platelet rich plasma to be re-injected into the face in hundreds of tiny needle sticks. In some states it seems this is being done, not by doctors but by licensed estheticians. It’s not hard to imagine what happens next. In New Mexico a cluster of 5 cases of HIV infection were traced to a “spa” performing this absurdity. Now you certainly can get an infection in a hospital or surgical center, but at least there they are making concerted professional attempts to prevent that. What other transmissible infections might you acquire through a carelessly conducted procedure where needles and blood are involved? Common bacterial infections like Staph, Strep or gram negatives could be devastating since the pathogen would be introduced into the skin of the face hundreds of times; Hepatitis C, and Hepatitis B, as well as HIV, are the viruses readily transmitted via needles. This reminds me of a cluster of horrific infections that occurred in Newark years ago. A number of women were infected with Nocardia (a nasty bug) after receiving silicon buttocks enhancement injections by a fellow who was not a physician, and sourced his silicon in the form of silicon caulk from Home Depot. The results were grisly requiring massive surgical debridement, and prolonged hospitalization for antibiotics. Don’t worry, the following picture isn’t from Newark but rather of a Vampire Facial. Caveat Emptor!

We all know that one of the biggest risk factors for severe disease or death from COVID is age, and a senescent immune system. Age related decrements in this biologic function increase our susceptibility to the widest range of infections, as well as cancer. Huge amounts of money are spent on countless supplements advertised to boost immune functioning, of course with no evidence whatsoever that they do anything other than lighten your wallet. A recent article in Nature provides some tantalizing suggestions that perhaps we are beginning to understand avenues that could lead eventually to therapeutics triggering the immune system to behave in a younger manner. The basic premise is that certain blood stem cells (primitive undifferentiated cells) are destined to develop into cells of the immune system that either enhance the body’s response to infections through the specific action of developing antibodies, called the adaptive arm—or into cells which ramp up inflammation in response to an invading challenge, called the innate arm. The research described here is conducted in mice, where it has been known that as the mice age the balance between these stem cells shifts toward a higher ratio of the inflammatory stem cells. We tend to think of inflammation as bad, and as we age increasing inflammation is indeed implicated in many of the sorry ailments that befall us. If you’re thinking why evolve the inflammatory cells in the first place, the reason is that the innate squad of immune cells act immediately upon detection of an intruder with a pre-programed set of responses that is effective for a wide range of insults. The adaptive arm is in charge of highly specific antibody and T cell responses which take much longer to get ramped up. With those preliminaries out of the way, these recent experiments in mice show that when antibodies targeting the inflammatory stem cells are given to the mice several things happen. The ratio of the two types of stem cells reverts back to that seen in younger mice, measures of inflammation decrease, and the old mice demonstrate enhanced immune responses to vaccination and resistance to viral infection. Very interesting cell biology and immunology here, but of course no immediate translation to potential human therapeutics. The link is below.
How to make an old immune system young again
https://doi.org/10.1038/d41586-024-00871-6
Final quick notes: The last continent reached by human beings was Antarctica, and the H1N5 Avian Influenza pandemic has finally reached there as well, with the virus being found in dead sea birds as well as sea mammals. This highly pathogenic influenza A strain has also just been identified in infected cows and their milk from several farms in Kansas and Texas. The cows are only moderately ill and will recover, and milk from them is being destroyed. Pasteurization should destroy the virus according to the CDC, but all bets are off with unpasteurized milk and milk products as a potential source of infection. I think we can add H1N5 to the list of other pathogens you can catch from unpasteurized milk for the foreseeable future.
The monoclonal antibody (MAB) nirsevimab was approved last August to prevent severe RSV in infants during their first RSV season. Real world data from the CDC has now confirmed that the MAB is performing in the post release “real world” just as well as it did in clinical trials, with 90% protection of infants against severe disease. RSV is the leading cause of infant hospitalization during the winter respiratory season and this is a major advance. Infants can also be protected when the mother receives RSV vaccination late in pregnancy. Interested readers are referred to the March 7th MMWR report
Early Estimate of Nirsevimab Effectiveness for Prevention of Respiratory Syncytial Virus–Associated Hospitalization Among Infants Entering Their First Respiratory Syncytial Virus Season — New Vaccine Surveillance Network, October 2023–February 2024
Weekly / March 7, 2024 / 73(9);209–214
Last on the agenda today is cause for celebration. Dr. Kocher’s Super Immune Blaster lozenges are once again available exclusively on the dark web. These immune rejuvenators will turn back the aging clock, and have your lymphocytes dancing like it’s the late 60’s. They are guaranteed to protect you from all known respiratory viruses, cure cancer, baldness and halitosis. The packaging states they are produced in a factory which processes nuts, stone fruit, seafood and fentanyl—so you know they are subject to excellent quality control. Hit the button at the bottom to order your lifetime supply—which will be much longer once you start on the program. Readers forwarding this publication will receive free shipping plus a one week all expenses paid vacation in Haiti. If you find the information in this blog useful, use the like button at the top.
Looking forward to receiving my Dr. Kocher’s Super Immune Blaster lozenges and my free 1 week vacation in Haiti 😄.