Quick Pre-Holiday COVID Update
First look at Real World Bivalent Booster Performance.

Sunny skies and snow covered slopes are calling, so I’m hoping to keep this brief, but cover the essential territory. COVID cases are continuing to increase across the country as a whole; no real surprise there, but at least we are not seeing the exponential rate of rise brought to us courtesy of Omicron, last January. Here is a CDC chart showing new daily hospitalizations have now topped 5,000/day with a continued week over week increase. As you can see we are now at about 24% of the peak daily hospitalizations during the initial Omicron wave.

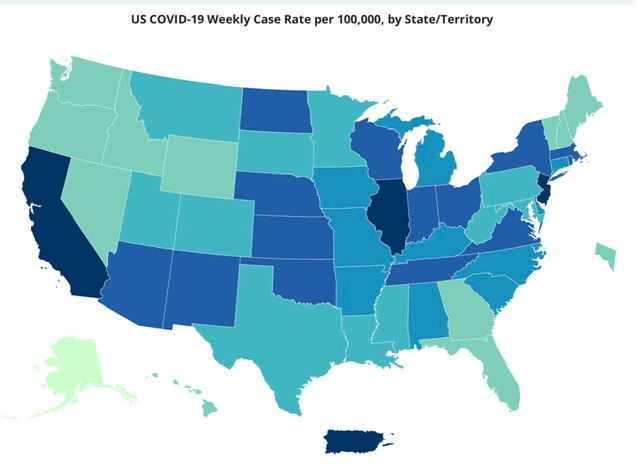
Below you will find a graphic, which those of us lucky enough to have gone to school without a year or more of “remote learning” will recognize as a map of the United States. It shows cases/100,000 population, and has the typical bicoastal pattern seen early in each of the COVID waves, with highest disease burden currently in New York, New Jersey, California and Illinois. As they like to say in the financial industry, “Past performance is no guarantee of future returns”, but a couple of years and rounds of COVID winter waves suggests disease peaks will follow shortly in areas of the US interior regions.
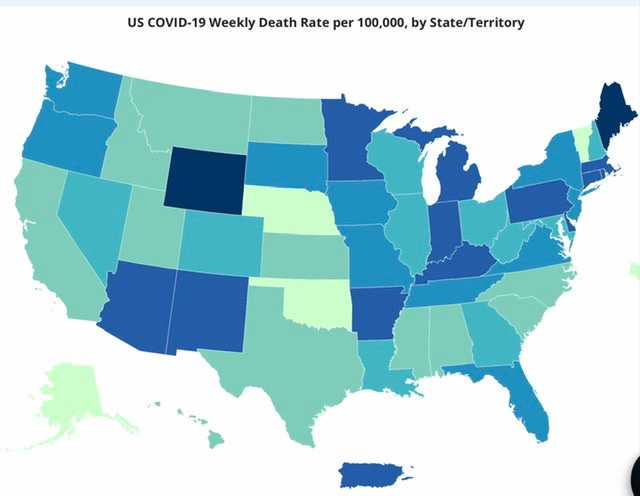
We all recognize that case counts are the mere tip of the disease burden iceberg, and below are current state population adjusted death rates. It does show an interesting situation, with the current highest death rates occurring in two states with polar opposite vaccination uptake—Wyoming on the low end and Maine with one of the highest rates. Maine also has one of the highest new bivalent vaccine uptake rates in the country. This is likely a statistical aberration based on a short observational timeframe, and higher disease burden currently in the Northeast—but that is merely a guess. For what it worth, Puerto Rico is in the highest current death rate category, with a full vaccination rate of 85%, which is among the highest.
This week we got very timely data from the CDC with a first look at the real world performance of the bivalent boosters, which first became available September 4th and with follow up through November 18th. The first data set compares the efficacy of a bivalent booster in all adults > 18 yo compared to either: no vaccination, or 2,3, or 4 doses of the original vaccine. The measure of VE (vaccine efficacy) is prevention of emergency medical treatment. Compared to no vaccination at all, the new booster offered 56% extra protection from requiring emergency treatment. Compared to prior vaccination alone, the new booster offered 50% increased protection if your last dose of original vaccine was 11 months or more ago, and 31% increased protection if your last dose was between 2-4 months earlier. How about protection from hospitalization? Compared to no vaccination, a dose of the new booster conferred 57% VE against hospitalization. If you were vaccinated and boosted in in the last 5-7 months, the new bivalent booster had an efficacy of 38%, and 45% if your last dose was more than 11 months ago. Keep in mind that the follow up here was only over 2 months, and we know that the protective effect of boosters falls off quickly beyond that point. The other issue to consider is that most of this trial reflects the efficacy of the new booster during a time frame when BA.5 (the virus they were designed against) was by far the dominant circulating variant. It wasn’t until the end of the week of October 22 that BQ.1 and BQ.1.1 became the dominant virus. Anyone wanting to bet that the BA.5 booster will perform better, or even as well against the new variants, I prefer new unmarked bills, and no Bitcoin thank you. If you want to delve into the details and statistical analysis look in MMWR Weekly Report of December 16th.
https://www.cdc.gov/mmwr/volumes/71/wr/mm715152e1.htm
Those results looking at all adults over 18 yo are not very impressive, in fact they fall below the threshold of protective efficacy that Dr. Fauci said early on would be necessary for a vaccine to obtain an emergency use authorization. He was speaking at that moment about the efficacy in preventing infection; we had not heard anything at that point in time about a distinction being made between preventing infection and preventing hospitalization. (That only came about much later, after the vaccines were widely distributed, and we saw that in the real world, and with the arrival of variants, that the vaccine’s ability to prevent infection was far below the 95% range advertised by the initial trials). The new booster’s VE in preventing infection will be WELL below it’s ability to prevent severe disease—perhaps the CDC has given up on measuring that metric. What about the bivalent booster’s efficacy in preventing hospitalization in the over 65 yo. age group—that’s were the beef is, these are the people going to the hospital today, and some dying. That data is presented in a separate MMWR paper from the same date, and if you only read the first one, you will miss out on important information. The good news here is that the booster’s VE looks BETTER in the over 65 yo. group, providing 84% increased protection versus being unvaccinated, and 73% protection compared to folks with 2,3, or 4 prior doses. I’m not at all clear on why the booster would be functioning more effectively in the older group. I could speculate that this group on average had fewer episodes of infection, due to behavioral factors, and thus less natural immunity compared to the younger folks. Perhaps their behavior today is lessening the intensity of exposure. Such factors might explain their increased benefit from the booster—but we have had enough speculation, often presented as scientific fact over the last three years. The results speak for themselves: the group at highest risk is getting the most benefit so far from the new booster, and it is at a very decent level.
The other bit of news this week, which I consider important, is the end of the military vaccine mandate. Back on February 18th I posted, “The Disappearing Vaccine Mandate”, and outlined all the reasons why at that point I considered COVID vaccine mandates illogical, unscientific and unnecessarily divisive. Despite regularly reading this blog, President Biden persisted with the vaccine mandate for the military, resulting in the dismissal of thousands of active military personnel, and apparently severely hampering recruitment efforts. As Commander-in-Chief any President can order you to do basically anything, ranging from the mundane, to heroic or stupid, as long as it does not violate a Federal Law. That Presidential vaccine mandate ended this week as the House and the Senate overwhelmingly passed a veto-proof bill making it illegal to order COVID vaccines for the military.
This week also saw New York and LA County officially enter the CDC high COVID risk category. There are of course nice suggestions that people wear masks, but it appears there is little likelihood of coercion at this time. The Governor of New Jersey said, “I don’t see any possibility of a return of mask mandates in New Jersey, not unless the hospital system is on the brink of collapse. We don’t want to mandate something we can’t enforce”. I suspect there will be some uptick in voluntary masking, particularly in the areas which were hard hit during the first COVID wave. Now is a good time to remember the “layered protection” theme.
Hope you have a great Holiday. There will be no update next week (barring a brand new Greek letter variant, war with China, or Sam Bankman-Fried asking me to join his legal team.
I’ve contacted him about a defense based on Long COVID brain fog, so we’ll see. Pass “Clear and Present Thinking” to your circle of friends and colleagues.