

Roll Up Your Sleeve, Again
What’s in a name—that it should smell so sweet?


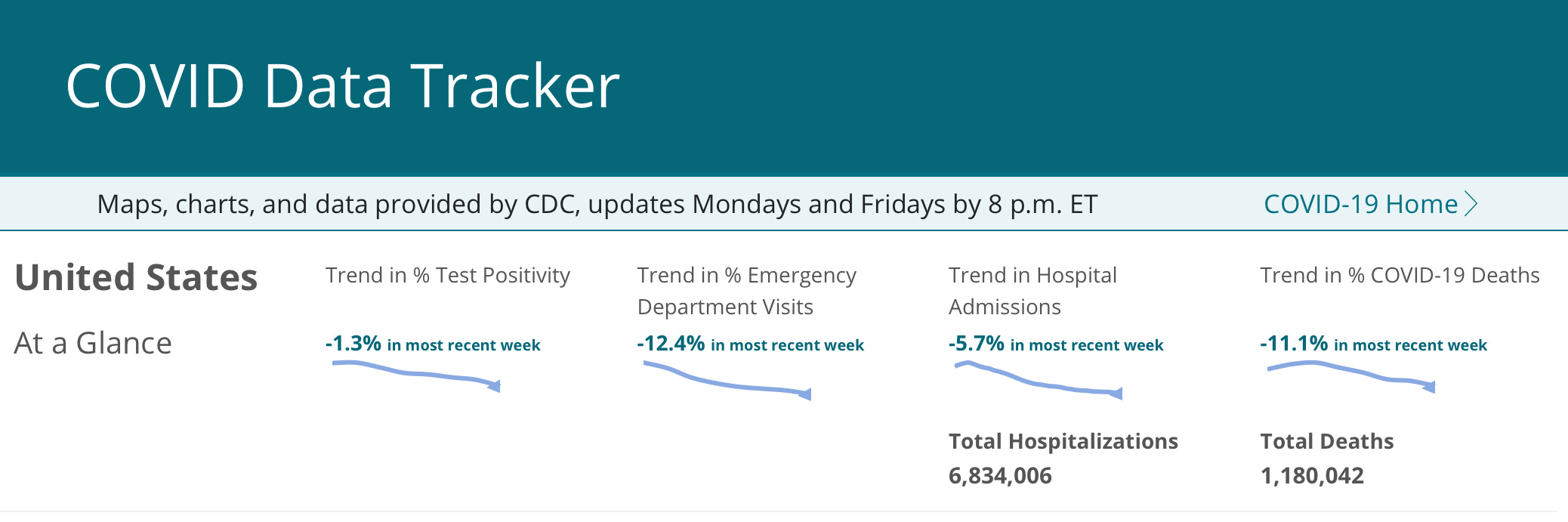
On Wednesday the CDC announced that they want people 65 and older, and those immunocompromised, to take another dose of the monovalent fall 2023 COVID booster this spring. This is prompted by data showing only a 40-50% effectiveness in preventing symptomatic infection and hospitalization. The CDC presented results showing that in October and November recipients of the fall booster were accounting for only 4% of hospitalizations—that sounds good, and obviously was communicated to try and rally enthusiasm, but we need to remember that at that point in time most of the newly boosted folks were probably 4 weeks or so after vaccination, and at peak effectiveness, which is rapidly waning. As I mentioned in a prior post, the majority of the data from which CDC calculated the 40-50% effectiveness was collected prior to the time in which JN.1 became the overwhelmingly dominant variant (currently 96% of sequences), and this virus has greater immune evasion than the strain the vaccine specifically targets. Although the winter surge of COVID is continuing to slowly recede, the CDC is rightfully concerned that 19,000 people a week are continuing to be hospitalized because of COVID, and this apparently figured strongly in their new recommendation. You might be thinking that the current iteration of the vaccine is no home run, especially compared to the effectiveness of the 2021 vaccine against severe disease. The “Warp Speed” vaccine targeted the original Wuhan virus, and it’s critically important to realize that the population at the start of the Pandemic had no immunity at all; thus the vaccine had little difficulty being extremely effective when deployed in this completely unprotected herd. Now virtually everyone in the country has some degree of baseline immunity from multiple vaccines and infections—that means that the booster’s effectiveness is being compared to unboosted folks with a great deal of existing immunity—you might look good playing tennis against someone like me (who doesn’t play at all), not so much against Djokevic. The most recent COVID statistics are below.
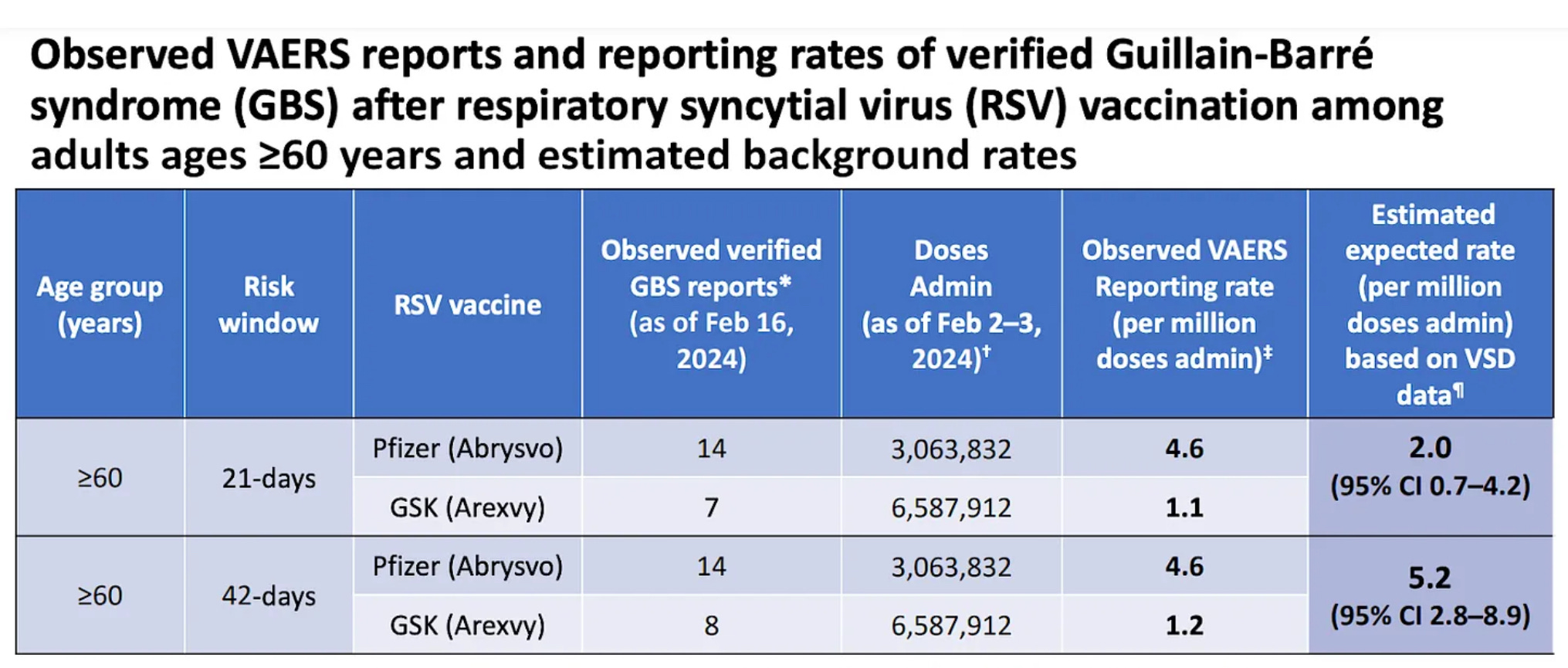
If you’re over 60, what about the new vaccine for RSV, which became available for the first time this year? If you have taken it, you are among the 16% of eligible Americans who rolled up a sleeve. There has been concern about a possible safety signal in the form of increased Guillian-Barre Syndrome (GBS) cases following vaccination, and perhaps you have been waiting for clarification of any risk. The Advisory Committee on Immunization Practices (ACIP) met this week and reviewed data collected by the CDC on this issue. The results from the VAERS system, which records vaccine associated side effects, shows there is indeed a mild safety signal for the two licensed RSV vaccines showing approximately twice as many cases of GBS syndrome as expected from the non-vaccinated baseline. These are very low numbers per million as you can see in the following CDC slide presented at the meeting. You will also notice that the GSK vaccine Arexvy, has a lower rate of this adverse effect than the Pfizer vaccine Abrysvo. Both vaccines seem to be maintaining very reasonable efficacy into the second year post vaccination. The CDC also presented calculations showing the benefit in terms of reduced hospitalizations and deaths greatly outweighs the slight increase in the neurologic side effect. The greatest benefit from vaccination is by far seen in the over 75 year old group. Younger people with pre-existing pulmonary disease are obviously at high risk, but so are especially those with chronic kidney disease, coronary heart disease, congestive heart failure and significant immune compromise. If you are a completely healthy person in your sixties I don’t think the risk benefit ratio argues much for vaccination. If you are at higher risk then certainly get vaccinated, and I would probably choose the GSK vaccine if there is an easy choice. Disclaimer: GSK has not provided me with any speaker fees, no show/no experience Board positions, gold bars, pre-paid escort services, or free buffets at Golden Coral.
RSVis a single stranded RNA virus, and something we haven’t seen discussed among all the public hoopla of the benefits of the new vaccine, is the potential for this RNA virus to mutate quickly under immune pressure from the vaccine. We saw very clearly with COVID, the other RNA virus in our lives, that once the population was immunized, selective pressure allowed the emergence of a myriad of variants, some of which quickly came to dominate the entire world. It’s my prediction that following wide spread adoption of the vaccine, which targets the two main strains of RSV, we will see the rapid emergence of immune escape variants. I don’t think it will be anything like the viral free for all of COVID; RSV has been adapted to humans for a long time, and has settled into an equilibrium with us. Since the vaccine is targeting only a fraction of the population, and uptake within that segment has been slim so far, that coupled with the short lived nature of immunity to RSV will ensure there is always a large group of susceptible hosts, and vaccine induced immune pressure should be relatively light compared to COVID. Public Health authorities have correctly made it clear right from the beginning that the vaccine for RSV is intended only to mitigate the severity of disease in a limited segment of the population at high risk. There is no talk of eliminating the virus, or preventing its spread to other people. That was not the message in the beginning with the COVID vaccines. If this sort of topic interest you, click on the link below to read a paper on the evolutionary dynamics of RSV in Argentina, the largest study of its kind ever.
Evolutionary dynamics of respiratory syncytial virus in Buenos Aires: Viral diversity, migration, and subgroup replacement | Virus Evolution | Oxford Academic https://academic.oup.com/ve/article/9/1/vead006/7003417
Next I want to look at the possibility that Brazil may be at risk for another epidemic of Zika related microcephaly and other fetal neurologic injury. I highlighted experimental evidence in a recent post that fetal neurologic damage from the Zika virus is dependent on pre-existing Dengue virus antibodies. Brazil is now in the midst of an enormous surge in Dengue disease. The country as a whole has registered a 4 fold increase in cases compared to the first 6 weeks of 2023 (which was itself a year marked by extremely high Dengue activity), and the Federal District of Brasilia is counting ten times the 2023 cases. The government has initiated the first country wide vaccination program with a newly licensed quadrivalent Dengue vaccine, which they are targeting at the 10-14 year old age group. They obviously picked this unusual vaccine specific group because it has been 10 years since the terrible Zika virus caused epidemic of microcephaly, and very young children at that time quite likely avoided mosquito born Zika infection. Those children are now approaching the age at which they might soon become pregnant. Given this huge outbreak of Dengue these young people can represent a significant group at risk for the now endemic Zika virus to hit with the potential for high level Dengue antibodies from recent infection. Just speculation on my part, but how else can you explain this unusual age group selection for a non-sexually transmitted vaccine campaign?
I have written extensively about the fact that the oral polio vaccine given out around the world by the WHO is now responsible for 99% of the paralytic polio disease occurring in Africa, South America, and Asia; and that only a tiny number of natural cases occur every year in only two countries. The WHO appears to have recently tackled this problem in classic bureaucratic fashion by rebranding what was previously known as “vaccine derived polio virus”, as “variant polio”. The scientific “justification” is that the live vaccine mutates endlessly in the gut of some recipients and is excreted in their stool where it can infect other people. We know from established data that children in third world settings have reduced response and hence protection from the oral vaccine compared to children in wealthier regions—and the WHO is not providing data on how many of the children with vaccine caused polio have previously received vaccination with the billions of doses that have been administered. The WHO maintains that the problem is under vaccination and poor sanitary conditions, but when virtually all the polio caused world wide is due to the vaccine they are handing out, isn’t it time to rethink the problem? Let’s be honest, the vast majority of people accepting this vaccine for their children don’t have the even a modicum of what we would call informed consent. If you were distributing a vaccine that caused 99%+ of the paralytic polio in the world, wouldn’t you want to rebrand it as “variant polio” rather than “vaccine derived polio virus”?
The editorial staff have recovered from their recent bouts of winter viral illness. The elite among them, (they all receive above the minimum wage) are building extensive underground bunkers, following the lead of many of the wealthiest tech billionaires in the country. Whether these bunkers are designed to protect from climate change, wide spread lawlessness, Right-wing or Left-wing politicians, nuclear war, day zero water shortages, the US default on its now 36 Trillion deficit, or the painful public use of inappropriate pronouns—their subterranean owners all love America, but just below the visible horizon.
Thanks for your time here, now go and enjoy the weekend and dig a little deeper into the science.
I neglected to reiterate that the polio vaccine in use in the US is the injectable inactivated vaccine, not the live vaccine. It never causes paralytic polio—vaccinate your children to protect them from visitors from parts of the world where the live vaccine is given.