

Science Whispers The Truth, Again
Pay no attention to those lights in the sky, and the government also requests that you don’t shoot down the drones

There have been quite a number of interesting items on the infectious disease front, and other areas of medical science in the last two weeks, and I will start with a study of the drug Tecovirimat, which was promoted by the NIH and the FDA for treatment of Mpox (Monkeypox). As you will recall when the Mpox epidemic started in 2022, the NIH recommended treating patients with this drug, which had been developed as a potential treatment for Smallpox—even though it had never been tested in persons with Mpox. There was some loud outcry about the inequity of infected people in third world countries not being able to access the drug. Well now we know, as a result of a randomized, placebo controlled trial, STOMP (Study of Tecovirimat for Mpox), that the drug works as well as hydroxychloroquine or Ivermectin for COVID—in other words NOT AT ALL. The data and safety monitoring board halted the study before completion of the full planned enrollment after they determined that the drug had no effect on lesion resolution time, pain, or progression of disease. This study was enrolling patients with mild to moderate clade II Mpox (the milder form of the virus which sped around the world via sexual contact), but as a result of the recent findings, the NIAID has also terminated an open enrollment study giving the drug to patients with or at risk for severe disease. Back to the drawing board, just when we have a new epidemic (not Pandemic yet this time) of the more virulent clade Ib Mpox raging in Africa. A much smaller randomized study of Tecovirimat for Clade Ib Mpox in Africa was reported this summer, and found the same complete lack of efficacy. Sometimes throwing spaghetti at the wall works, and sometimes it doesn’t. The question of whether a therapy is effective or not is never answered by treating physicians’ enthusiastic endorsements based on observational studies, or the recommendation of experts based on reasonable scientific evidence from the laboratory. The urge to “do something now” in an emergency situation is an innate human reaction, perhaps not all that different from the flight or fight response, and compounded in the political arena where a perceived lack of response and control of the situation is the kiss of death. If you are interested in the truth about the material world, the scientific method reliably comes through. If you want the “truth” in the social, political, or metaphysical realm, then pick your poison.

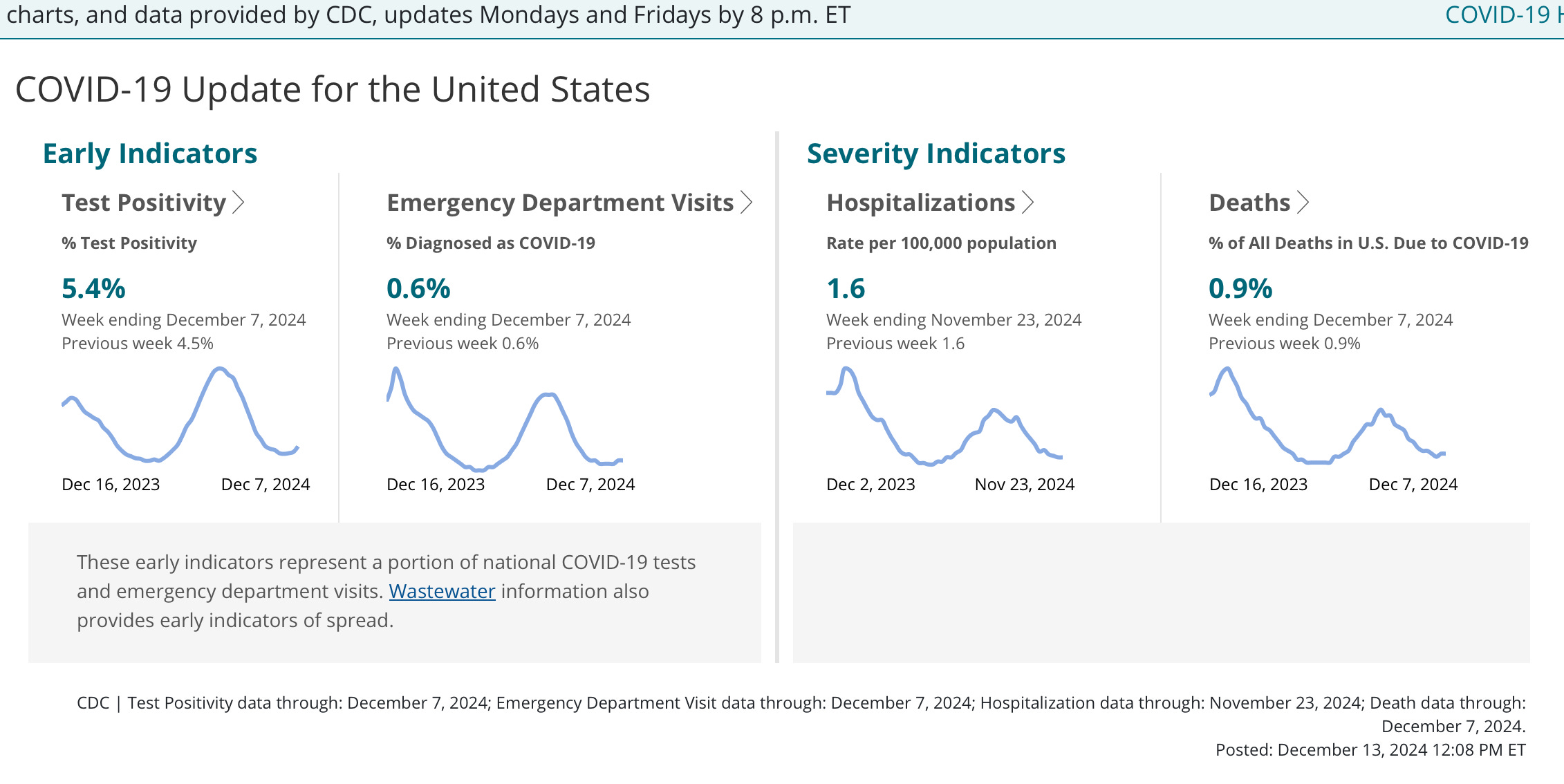
Has COVID lost its mojo? Maybe the Omicron family of the virus is running up against a wall of human immunity that is crimping its style. We have not seen the typical post Thanksgiving increase in disease, which usually would have set in by now. There is a small increase in test positivity, but so far no significant bump in emergency room visits or hospitalizations. Fingers crossed for the main winter season, but I wouldn’t count this virus out ever. The other major respiratory culprit Influenza is also off to a slow start this year, with US national levels remaining low both in the waste water and in clinics. RSV is demonstrating a somewhat unusual pattern where emergency room visits have increased to a moderate level while my favorite metric, waste water levels have remained low. The vast majority of patients presenting to ER and hospital right now have been very young children, and I think the RSV virus is getting tossed with the diapers, and not making it into the usual waste stream.
Here is an example of “received wisdom in medicine”, as I like to call it, failing at the test of rigorous study. We all know that high blood pressure is bad for you; when a patient in the hospital has episodes of elevated blood pressure it has been “standard medical practice” to treat it with medication. As a young physician in training I might have been criticized for failing to treat a hospitalized patient’s moderately elevated blood pressure. But hypertension is a condition that causes increased morbidity and mortality over the course of decades, and hospitalized patients under stress of illness or pain may be having temporary elevations in blood pressure. Does treating those elevations in blood pressure with an “as needed” medication benefit them? Perhaps a particular patient may even have undiagnosed true hypertension, but is the best time to start treating it when they are acutely ill from some other pathology? A recent retrospective study of 133,700 hospitalized veterans seems to indicate that, at least in this older population, such treatment is associated with a 23% increased risk of acute kidney injury and a 50% increased risk of rapid (and greater than desired) blood pressure drops. Yes it’s a retrospective study showing an association, but the mechanism of injury makes sense, and there is zero evidence from any kind of study ever showing a benefit from this kind of intermittent treatment initiated in the setting of hospitalization. I believe all studies showing a benefit for treatment of hypertension are in the setting of long term out-patient treatment.
Canales MT, Yang S, Westanmo A, Wang X, Hadley D, Ishani A, Mohandas R, Shorr R, Lo-Ciganic W. As-Needed Blood Pressure Medication and Adverse Outcomes in VA Hospitals. JAMA Intern Med. 2024 Nov 25:e246213. doi: 10.1001/jamainternmed.2024.6213. Epub ahead of print. PMID: 39585709; PMCID: PMC11589853.

Sacred cow deemed free from H5N1, and also free from testing by scientific method
A fascinating article regarding the skin’s contribution to the functioning of the immune system appeared this week in Nature. It has been known for some time that the immune system of humans and mice respond to the presence of the commensal bacterium Staphylococcus epidermidis on the skin by production of a vigorous antibody response—in the absence of any infection. It has also been shown that immune cells in the skin (Langerhans cells) are capable of initiating both local production of antibodies within the skin, and also triggering the deeper response of antibody production within lymph nodes, so that systemic antibodies to the organism are formed in the blood, and at other mucosal surfaces (IgA class antibodies in the mouth, respiratory, and GI tract). The current investigators took Staph epidermidis and grafted a fragment of tetanus toxoid protein onto one of the surface proteins of the bacteria, and then introduced the altered bacteria into the surface microbiome of the mice. Without any infection being caused, the mice produced high levels of neutralizing anti-tetanus antibodies, and the treated mice were able to survive a dose of the tetanus toxin which was lethal to all the control mice. The investigators also showed that other immunogens could elicit a similar response. Perhaps down the road we could be looking at immunization with something applied to the skin, skipping the needles, the local painful reactions, and maybe even the systemic symptoms of fever and malaise. Nice to contemplate, especially for the kiddos. A link follows if you have greater interest.
https://www.nature.com/articles/s41586-024-08489-4#citeas Discovery and engineering of the antibody response to a prominent skin commensal
The following event reported in Newsweek and other international sources is certain to boost your confidence in the ability of biological research laboratories, and the people who operate them, to safely contain highly lethal pathogens. It seems that a government research lab in Queensland Australia lost HUNDREDS of vials of live Hendra, Hanta and Lyssavirus samples. I won’t go into the details about these viruses other than to say that they are incredibly lethal to humans. The authorities in Australia believe they may have gone missing in 2021, but confirmed it only this August, in what the Minister of Health described as, “A most serious breach of lab biosecurity”. They say there is no evidence that these vials were stolen (could a thief possibly have forgotten to leave a thank you note?) and paint the cheerful picture that they suppose the vials must have been moved when a refrigeration unit failed, but by gosh they can’t find them anywhere. When anyone tells you that scientists need to artificially engineer viruses to make them more lethal and capable of infecting humans, and that because these scientists are such very responsible and clever persons, nothing could possibly go wrong, or leak from a lab—tell them you are a hard core conspiracy theorist, and two more things. You don’t appreciate people in positions of public authority telling you to ignore common sense and your own lying eyes, and that they need to seek other employment.

As we continue to monitor H5N1 Avian Influenza’s march through the mammals, and its adaptation to human transmission, the CDC has concluded that a California child with illness after consuming raw milk does NOT have Avian Influenza. (That may or may not be a correct conclusion, since apparently only very low levels of virus were recovered from the child making it difficult to firmly characterize.) Another youngster in California who did contract H5N1 last month had no identifiable risk factor or exposure. This week the CDC announced the first case of severe Avian Influenza in a resident of Louisiana. This is in an older person hospitalized in intensive care, and associated with exposure to a backyard flock of poultry. I have been waiting for news of the outcome of the case of the teenager in Canada who was critically ill and hospitalized in ICU with H5N1 back in November—but inexplicably the Canadian Provincial Health Authority is refusing to provide any further details about the case, citing “privacy reasons”. The reporting initially was of course anonymous, and this about-face is incredible. The pathetic US response in the early stages of the H5N1 spread to dairy cattle last spring has been criticized by scientists around the world, not only for its inept, torpid approach, but for a lack of transparency and information sharing. Looks like the Canadians may be competing for international acclaim. On a brighter note the US government has finally ordered mandatory testing of all unpasteurized milk for H5N1. Raw milk is legal in one way or another in all but four US states, with California being the largest producer, so the potential for human exposure is huge.

Returning to the theme of, “How safe is the food supply?”—Red Dye #3 is found in hundreds of food products that Americans consume. It is derived from petroleum, known to be carcinogenic in animals, thought by many scientists to be carcinogenic in humans, and banned in the EU. The FDA banned the use of RED #3 in cosmetics and medicated lotions and ointment way back in 1990, but decided in another separate review that you should continue to enjoy it in your food. Now with unsurprising timing, the FDA says it will respond to another petition to ban this chemical, and a decision “will come soon”. Red Dye 40 has been linked to neuro-behavioral problems in children by multiple studies, and in 2007 UK food authorities agreed it was a danger, but instead of banning this colorful agent, the EU countries put a warning label on any food containing it. Our FDA held a meeting in 2011 of its food science advisers who narrowly objected to either banning the dye or issuing an EU type warning label. Another meeting of FDA scientists in 2019 came to the conclusion that only a “sensitive subset” of children are subject to the neurologic ill effects of Red Dye 40, and California’s EPA came to the same conclusion about this dye in 2021, but of course it still remains in our diet, giving its fluorescent color to hundreds of food and beverage products. The FDA argument against banning these and other suspect additives is that multi-billion dollar food business are entrenched in their use, and that the FDA just doesn’t have the iron clad proof of harm to fight the industry lawyers in court. Funny how kids in Canada, Australia, and all of Europe still gobble down their Fruit Loops and Gatorade, even if they no longer glow in the dark. Just my guess, but I’m betting that very shortly we will see a whole list of chemical adulterants removed from foods—and a list of politicians who have been in power for years climbing over each other to claim credit for this.
Here we are at the Holiday Season again with events from around the world bringing us tidings of great joy. New York and New Jersey have been subject to nocturnal displays of moving lights for weeks now. At first the Federal Government declared that there were no drones, and people were seeing only commercial aircraft. That story evaporated after an airport in upstate New York was closed for hours as it was besieged by the objects. (Seems airports can tell pretty clearly whether commercial or private aircraft are flying around them, and they may have filled Washington in on that information.) Now following calls from the two states Governors, 21 Mayors in New Jersey, multiple Congressmen and both states Senators, the Biden Administration says that the FAA, FBI, NSA, and Homeland Security are hard at work seeking an explanation for the drones, that they are undoubtedly harmless, and asking residents not to shoot them down. At a top secret briefing for some Congressional members on Monday it was revealed that so far the investigation has ruled out new prototypes of Santa’s sleigh, a search for missing radioactive medical waste, swamp gas….but not gas-lighting.
As the year winds down I want to thank everyone who reads, “Clear and Present Thinking”, and passes it on. Kudos for pounding the like button as well. Also I would like to remind you that I am selling several of my prized Hunter Biden original oil paintings, now at a 95% discount from original purchase. This personal collection was amassed several years ago, when I was hoping to be nominated for the position of Surgeon General, but I was passed over in favor of a connoisseur with deeper appreciation of art, and pockets. The market has shifted recently, so your good fortune awaits—needing only the sending of some Bitcoin to my Cayman Island account. Merry Christmas and Happy Hanukkah.
AFAIK, Red Dye 40 is not completely banned in any of the regions you mention, but it is subjected to varying levels of regulation and restriction. For example, the EU has stricter labeling requirements and a lower ADI.
I think as medical providers when one is encountered with an infectious disease where there is really no good treatment for that our hearts sometimes take over logic as we don’t want to see our patients die. I think back to the onset of Covid and the multiple changes of treatments over the two years and the heartbreaking of trying everything and “throwing the book at “to try and save a person to no avail. And the changes that occurred over those 2 to 3 years to include prone or not prone,, steroids are not steroids, antivirals, plus steroids, etc., etc. more recently my daughter‘s coworker who is my daughter‘s age and has been immunized who got Covid but was otherwise healthy and within about two weeks was on hospice and a week later had died. I think about all the advances of modern medicine how we truly can’t save everyone, but we do our darndest to try and save them. I agree that randomize controlled trials are the best but sometimes they just don’t come quick enough but ultraviolet light, etc. that was recommended by the Trump team was a laughing joke.