

The Chinese Have a New Exciting Corona Virus
What could possibly go wrong?

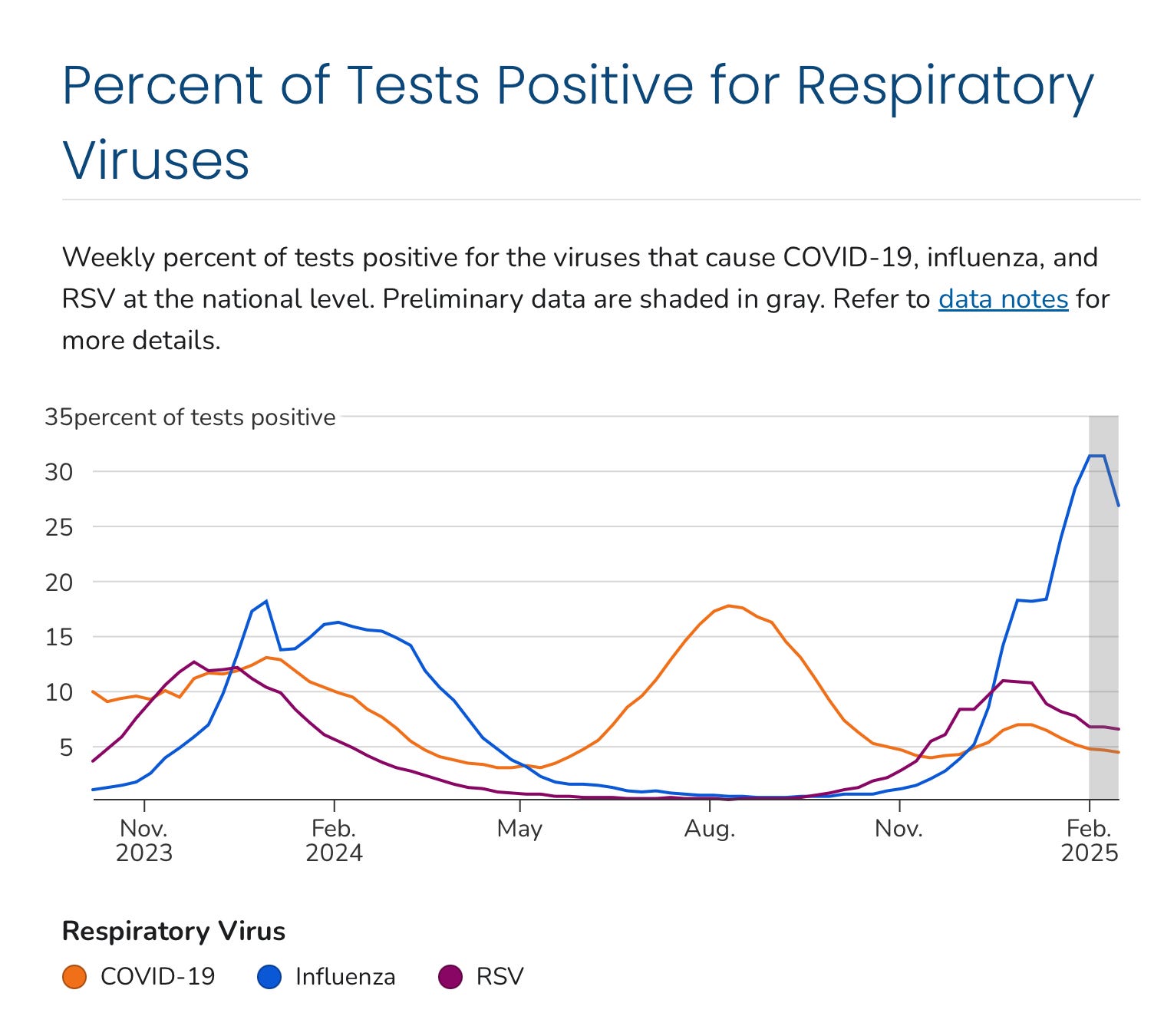
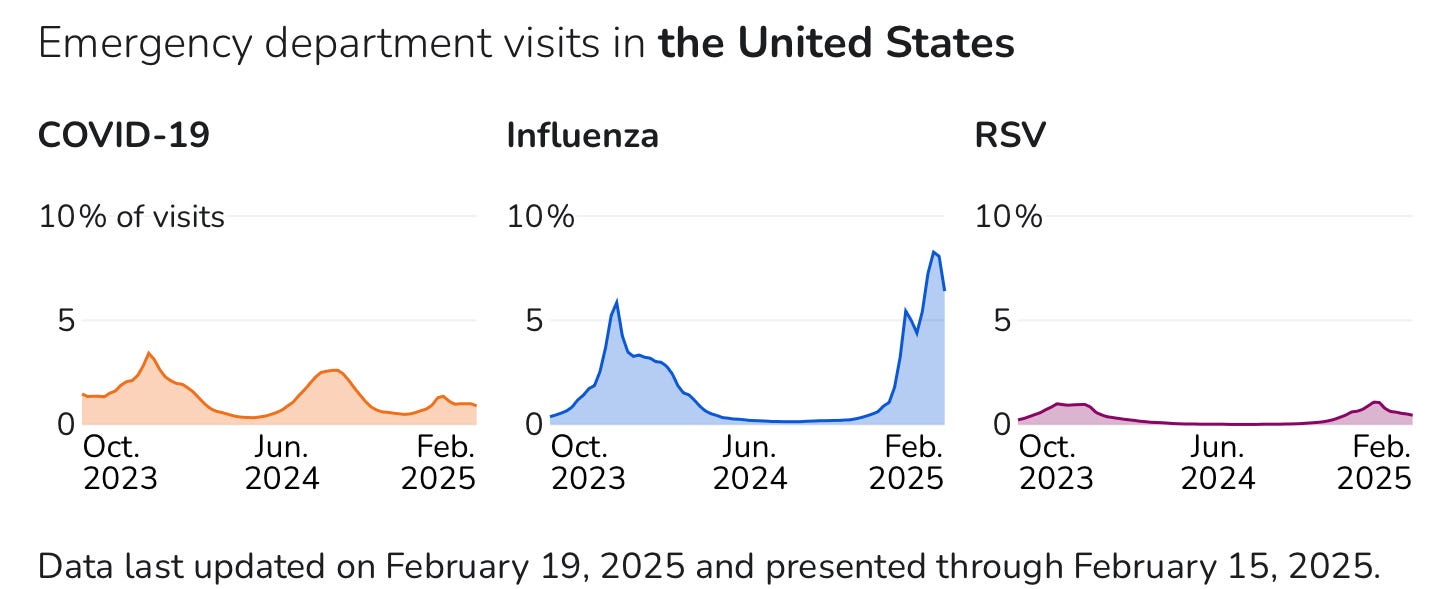
I’ll start with a quick follow up on the winter respiratory virus season. Back in December I suggested that COVID was looking like it didn’t have the mojo this year to cause a significant winter wave, and for the first time in five years that turned out to be the case. On the other hand, Influenza has been having a banner year, and almost all the folks you know who have been sick over the past 6 weeks have had the flu, and very few COVID or RSV. It looks like Influenza peaked and began a slight decline in the second week of February, but late secondary peaks are not unusual with this virus—so stay tuned. The first graph highlights what a great proportion of respiratory illness has been due to Influenza this winter—a stark contrast to the first several years of the SARS2 Pandemic. Influenza hospitalizations this year have surpassed those recorded in the quite severe pre-pandemic 2018-2019 season. The second graph shows that all this Influenza is having its impact on emergency room utilization. It’s interesting that the summer COVID wave this year was much greater than in the winter; the virus simply refuses to settle into a simple seasonal pattern like many other respiratory pathogens. The surges in disease activity are driven by a host of factors, including not just increased indoor congregation, but the emergence of new variants at unpredictable times, and the rapid waning of prior immunity sufficient to prevent infection. Taylor Swift concerts, SNL fifty year celebrations and White House events of either party also make the list.
A surprising number of the general population are now attuned to what’s new and interesting in the world of Virology—well at least, what’s new and potentially life disrupting, or pandemic inducing. Our friends at the Wuhan Lab in China have just reported a newly identified corona virus, which they have named HKU5-CoV2. As usual this is a virus that they teased out of bats in remote caves in southern China; something that might not be expected to have much opportunity to intersect with humans, other than the Chinese researchers plumbing those caves up to their knees in bat guano, and of course the people back at the lab. This particular corona virus belongs to the family of the MERS virus (Middle East Respiratory Syndrome) a merbecovirus with an enormously higher mortality rate than SARS2 (COVID). The new HKU5-CoV2 virus utilizes the same ACE2 receptor to infect human (and other mammalian cells) as SARS2, and replicates well within those human cells and respiratory organoids (tiny artificial groups of human cells that simulate the human lung or other organs).
https://www.cell.com/cell/abstract/S0092-8674(25)00144-8
Bat-infecting merbecovirus HKU5-CoV lineage 2 can use human ACE2 as a cell entry receptor
Now that the Wuhan Lab has recovered this virus from nature, can we trust them not to go tinkering with it to enhance its infectivity or pathogenicity—aka Gain of Function Research. We know (despite the denial of the former director of NIAID) that they were doing just that with corona viruses closely related to SARS2 when the Pandemic arose in Wuhan in late 2019. We also know that our own scientists and intelligence services evaluated the safety of the lab’s containment apparatus and protocols and found them to be severely deficient. Surely the Chinese must have corrected those deficiencies. Even if you believe there is only a 50% or 25% chance the Pandemic arose from a leak at this lab, you must believe that they would never make the same mistake twice. If you’re thinking that because this virus attaches to the ACE2 receptor, antibodies we have from the Pandemic, which bind to the SARS2 RBD (Receptor Binding Domain) may block this new virus from attaching—that is not going to happen. The paper above demonstrates HKU5-CoV2 attaches to the receptor in a completely unique way, not seen with prior corona viruses, consequently our antibodies to all the iterations of COVID would almost certainly be useless.

I have opined repeatedly that there is no solid scientific evidence to support the CDC and the ACIP continued recommendations to vaccinate young children with yearly COVID boosters. Absence of evidence of course doesn’t prove me right, but this study just published in the Journal of the Pediatric Infectious Disease Society certainly provides some solid evidence to support my view. (It’s not just my opinion, as I have recently pointed out, but the conclusion of the vast majority of parents in the US who have given boosters to just 10% of children the CDC recommends receive them). The current study from San Francisco looked at three cohorts of children less than 5 years old during the early Omicron variant period, monitoring the children closely for both asymptomatic and symptomatic COVID infection by PCR sampling (and sequencing). Broadly, their conclusions were that prior infection (of any remoteness in time) was the only determinant of a reduced chance of infection. Vaccination alone had no effect.
SARS-CoV-2 Risk Is Lower Among Young Children With vs Without Prior Infection
Regardless of the timing of prior infection, individuals with vs without evidence of prior SARS-CoV-2 infection were less likely to be infected with SARS-CoV-2 (hazard ratio [HR], 0.28; 95% CI, 0.16-0.49) and experience symptomatic COVID-19 (HR, 0.21; 95% CI, 0.08-0.54).
No differences were observed in risk for infection or symptomatic COVID-19 by vaccination status alone, regardless of vaccination timing or vaccine manufacturer.
Compared with unvaccinated patients without previous infection, patients who received a Pfizer-BioNTech vaccine and did not experience previous infection were more likely to be infected and experience symptomatic COVID-19 vs (HR, 2.59; 95% CI, 1.27-5.28). In contrast, patients who received a Pfizer-BioNTech vaccine and did have a prior infection were less likely to be infected (HR, 0.22; 95% CI, 0.05-0.95).
Make what you will of the statistically significant finding that vaccinated children without prior infection were more likely to become infected than non-vaccinated kids also without prior infection. I’ll chock that up to a statistical aberration which might disappear with a larger sample size—but alternative explanations might invoke changes in parentally controlled behavior, with more varied social exposure, or worse. If you are an academic pediatrician or epidemiologist, this is not the result you were expecting, and predictably the authors fall back on the mantra: “COVID-19 vaccines are recommended to reduce severe illness; overall risk of infection may not differ substantially between vaccinated and unvaccinated children <5 years.” (my highlighting)
I have not written much about long COVID, frankly much of what gets published I consider to be of such poor quality, murky psuedoscience, that it has contributed almost nothing to our fundamental understanding of the problem. That is despite the NIH receiving over a billion dollars to study Long COVID in 2020. Much of that money was wasted in repetitive symptom based correlation studies. More of the money was spent measuring and cataloguing all sorts of parameters of the immune, inflammatory, and neurologic systems; which have provided no real understanding of the basic pathophysiology or effective treatments. (Anyone with an assay that could measure anything at all related to these systems has been busy turning out papers). The following study falls into a completely different category. One of the theories of Long COVID etiology is persistence of viral replication in areas of the body sequestered from the full reach of the immune system. Earlier attempts to measure this were hampered by questions about the sensitivity and specificity of the assays employed, very small sample sizes, lack of accounting for vaccination or re-infection, and lack of adequate control groups. Also, reports of well documented viral persistence during acute infection in immune-compromised people are very interesting, but not widely applicable to the problem of Long COVID in otherwise normal people.
Plasma-based antigen persistence in the post-acute phase of COVID-19
Michael J Pelusoa,† michael.peluso@ucsf.edu ∙ Zoe N Swanke,f,g,† ∙ Sarah A Goldbergb,† ∙ Scott Lub ∙ Thomas Dalhuisenb ∙ Ella Borberge,f,g https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(24)00211-1/fulltext
Rather than look for traces of the virus’s genetic material in plasma or tissue, these investigators looked at viral proteins in the blood of 171 recovered COVID patients at time points up to 14 months. To address some of the problems mentioned above, they studied frozen blood samples from patients early in the Pandemic, when vaccination and re-infection were not confounders. They validated the specificity of their protein assays by using control sera from 250 people taken before the Pandemic—the low levels of reactivity seen in this group defined the specificity or baseline cross reactivity to proteins in the blood of normal people unrelated to COVID infection.
Of 660 pandemic-era specimens tested, 61 (9·2%) specimens from 42 participants (25% of the group), had one or more detectable SARS-CoV-2 antigens (figure A). The most commonly detected antigen was spike (n=33, 5·0%), followed by S1 (n=15, 2·3%) and N (n=15, 2·3%). Compared with the pre-pandemic era participants who had 2% assay positivity, detection of any SARS-CoV-2 antigen was significantly more frequent among the pandemic-era participants at all three timepoints in the post-acute phase of infection (figure B–E). The absolute difference in SARS-CoV-2 plasma antigen prevalence was +10·6% (95% CI +5·0 to +16·2) at 3·0–6·0 months post-onset of COVID-19; +8·7% (+3·1 to +14·3) at 6·1–10·0 months; and +5·4% (+0·42 to +10·3) at 10·1–14·1 months (appendix p 11).
You can review the details of the study via the link to this paper in Lancet if you are inclined. I consider it pretty remarkable that they found SARS2 viral proteins in the blood of 8% of people 6 to 10 months after recovery, and 5.4% of people out at 10-14 months. Finding protein antigens in the blood, rather than fragments of viral RNA in tissues, increases the chances that ongoing viral replication is present, and perhaps responsible for Long COVID in at least a subset of people suffering from this, and also a reasonable mechanistic explanation for the finding of elevated inflammatory markers and markers of persistent immune activation. The next logical step would be to apply this methodology to study a group of people with fairly well defined Long COVID, and compare them to normally recovered individuals without persistent symptoms.
A small number of people have complained about a variety of chronic symptoms following their mRNA COVID vaccinations, and the symptoms reported are very similar to Long COVID. Many of these people were initially dismissed, but over time were taken more seriously, and the term Post Vaccination Syndrome (PVS) has been applied. A paper regarding this syndrome from a Yale lab in pre-print form just a few days ago has created quite a bit of attention in the press, and I think it’s worth noting, if only for a possible relation to the previous discussion of persistent COVID proteins in the blood. The researchers studied patients with PVS and compared them to normal controls. They found all sorts of differences in measured parameters of the immune system between the two groups which I won’t go into, but a subgroup of the PVS cohort was found to have much higher levels of the vaccine induced COVID S protein (Spike) circulating in the blood for prolonged periods, up to 700 days post vaccination. This wasn’t supposed to happen, but then you never discover extremely rare side effects of vaccines or medicines until after they have been approved and given to millions of people. Not all the PVS folks had this finding of persistent high level S protein in the blood, so its causative role in their symptoms remains to be determined—but now we know something important about how this vaccine interacts with a tiny percentage of people.
Immunological and Antigenic Signatures Associated with Chronic Illnesses after COVID-19 Vaccination MedRXiv Feb.18, 2025 https://doi.org/10.1101/2025.02.18.25322379
Closing out the vaccine section today I will point to an absolutely fascinating paper, again from a research group in San Fransisco, as an example of how people shouldn’t waste time and money on useless “scientific investigations”.
Substantial Gaps in COVID-19 Vaccination Exist Among People Who Inject Drugs https://www.vaccineadvisor.com/news/subtantial-gaps-in-covid-19-vaccination-exist-among-people-who-inject-drugs/
This study discovered that people who regularly inject drugs, get fewer COVID vaccines than non-drug users—who could have guessed. They also found that testing positive for COVID was MORE common among those who had been vaccinated. Now you don’t suppose that an iv drug user who has had some contact with a source to give that person a vaccine (be it health care or incarceration) is more likely to get a COVID test, whether they are sick or not?). The link is provided only as assurance I didn’t make this up.
Thanks for spending your time reading “Clear and Present Thinking”. Think of a few people you know who don’t get enough junk in their in box and then forward this. The like button at the top can be tricky but very rewarding—I’m told that the FBI no longer monitors it for subversive types, but you never know.
I sincerely wonder whether the motive here for ccp is a method to significantly mitigate their crippling demographics time bomb which, if left unchecked, gives them an absolute ceiling in terms of great power ascendancy. This is their one real serious issue, in terms of eventually surpassing a decaying America which seems hellbent on weakening its most critical security alliances just in time for China to achieve true parity. The pandemic leak path provides ccp at least some plausible deniability, is repeatable, and disproportionately affects the aging and elderly. Food for thought.