

The Right Stuff?
What’s in your needle?

I don’t usually present anecdotes, but I’ll give this one a pass since it might illustrate a helpful bit of science. It’s that time of year again when you are either salivating for your next COVID booster, or getting hot under the collar about the endless messages suggesting you had better take the jab— if you know what’s good for you. Perhaps you are like me, and had fairly miserable reactions from your last two COVID boosters, and opted to skip a year. I then decided to take a half dose of Moderna’s mRNA last December, and had zero reaction. I have remained COVID free since my first infection with the initial wave of Omicron over two years ago. My decision was based on zero data relating to this particular vaccine, just the general principles of immunology which tell us that repeated exposures to an antigen lead to very rapid and high level antibody responses (anamnestic response) even to smaller amounts of the antigen than the initial exposure. Now there are results from a well designed trial in the Netherlands looking at a related scenario. These researchers gave boosters of mRNA at a 5 fold reduced dose to previously normally vaccinated people with a history of prior allergic reactions. The doses were given into the skin (intra-dermal) rather than the standard IM (intra-muscular), which is an important difference. They found that the reduced dose group mounted as high (or perhaps slightly higher) antibody response as historical control groups with similar vaccination history—and they had much reduced allergic reactions. This is the same approach used with the Jenneos Mpox (Monkeypox) vaccine at the beginning of the 2022 Mpox pandemic, in order to stretch the very limited supply of the vaccine. That public health decision was made without specific data on its efficacy, but based on sound reasoning—just like my personal “experiment”.
Roozen GVT et al. Intradermal fractional dose vaccination as a method to vaccinate individuals with suspected allergy to mRNA COVID-19 vaccines. Vaccine. 2024. 42(25):126093. https://doi.org/10.1016/j.vaccine.2024.06.060
You are probably thinking how could I convince my own vaccinator to let me try this approach? You might be able to sell the idea to your personal physician if you have a solid relationship, but good luck trying that at CVS, Walmart, or Fred’s vaccination stand at the gas station. There is another approach to consider, if you are really in a high risk group, and are considering skipping the shot this fall because of rather bad reactions in the past. This gives me an excuse to relate another anecdote. My editor had increasingly severe reactions to COVID boosters, and with the last mRNA two years ago she developed fever, fatigue and very large, painful lymph nodes in her axilla which persisted for a week. She decided to take the Novavax protein-based COVID booster this week, and had zero reaction. It just might be the case that your immune system isn’t racing into overdrive because of the COVID spike protein itself, but rather an over-reaction to RNA (which is seen as a danger incoming VIRUS alert).
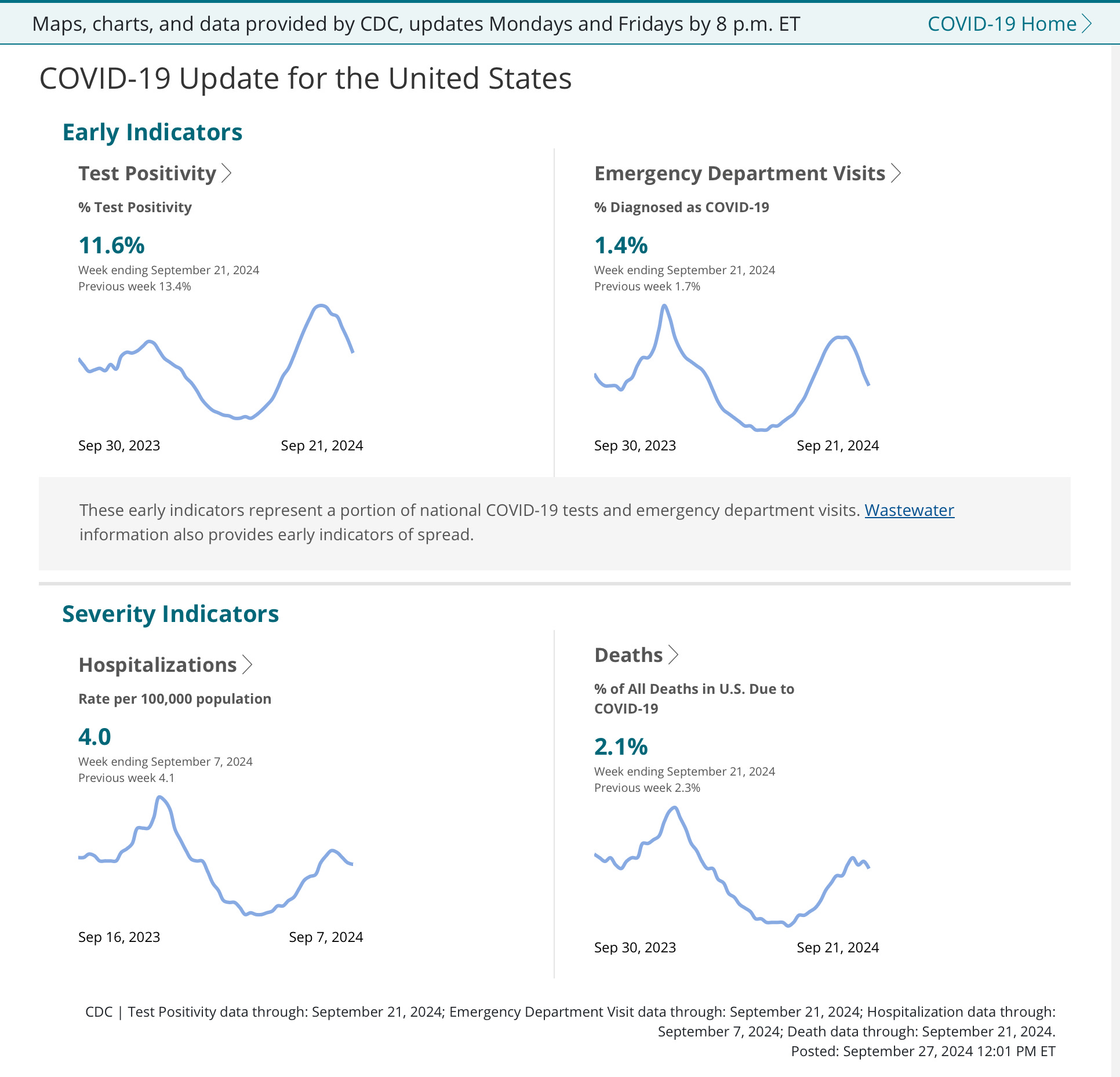
The COVID summer wave, larger and longer lasting than previous years, is finally beginning to recede as the following CDC graphs will show. Although COVID wastewater levels are still in the high or very high range in 40 states, the virus is declining in 22 states and stable in the rest. Let’s not loose sight of the fact that although COVID for most people now is just a cold or mild flu-like illness, that 56,000 people died from the virus during the past year. Any brand new, suddenly appearing disease with that kind of kill record would generally be considered a catastrophe, but put into the perspective of the last 4.5 years it’s only 1/6th of the number of US citizens dying during the first year of COVID. Once a again, as usual, we are entering the vaccination season with a COVID vaccine designed around a specific variant which is already almost extinct. The good news is that the current dominant variant KP.3.3.1 is close enough in structure to the vaccine variant that we can expect the usual fairly good protection from severe and fatal disease, but mediocre and relatively short duration of protection from infection.
If you have been reading the newspaper you might be aware that a new COVID variant XEC is spreading rapidly in several European countries. This is another recombinant variant, which presumably arose in a person simultaneously infected with two different COVID strains. XBB, a blast from the past which rapidly became the world-wide 2023 dominant variant, was another example of this recombination process. Although XEC is less than 1% of sequenced COVID virus in the US, it has rapidly become 16% in Germany and perhaps 7% in the UK. This variant looks to have increased immune evasion and a definite growth advantage over other current strains. I will provide a link if you have a curiosity as to the particular mutations felt to be responsible; but XEC is a combination of two strains descended from COVID variant JN.1, which have been in circulation since the beginning of this year, and although it may end up driving the upcoming winter surge, we should have plenty of partial immunity to guard against a major wave of severe illness. Remember that a repeating pattern of this Pandemic has been the spread of new COVIDS from Europe and the UK to the East Coast and then steadily across our country.
https://theconversation.com/xec-what-you-need-to-know-about-the-new-covid-variant-239125
Measles is once again on the rise with a large outbreak in the Twin-Cities area of Minnesota. The current outbreak is almost exclusively affecting the Somali population there, and 85% are in unvaccinated children (the vaccination status of some of the others is unknown, so it is quite possible nearly every case is occurring in the unvaccinated). This statement from the state’s head epidemiology officer sums up the seriousness of this frequently severe and sometimes fatal illness. Let’s keep in mind that local spread of measles was nearly extinct in the US a few years ago.
In an interview with MPR News last week, Dr. Ruth Lynfield, the state
epidemiologist, said Minnesota's total number of confirmed cases in
2024, which is 58, is as many cases as the entire United States
recorded in 2023.
We are waiting for the CDC to do serologic testing on contacts of the human case of H5N1 Avian Influenza A, which occurred without animal contact. Several of those contacts had flu-like symptoms, but were not tested for the virus while they were symptomatic. That leaves the option of testing them in a few weeks to see if they have developed high levels of antibody against the particular clade of H5N1 which infected the index patient. Let’s hope not, because adaptation of the virus for human to human transmission will dramatically up the risk for a very serious pandemic. In the meantime, some researchers from Texas have just reported in the New England Journal of Medicine the disturbing finding of H5N1 in the wastewater from 10 of 10 cities they monitor, 21 of 22 sites and 100 of 399 samples. With no increase in clinical influenza activity, we have to assume this is coming from a variety of animal sources. The ubiquitousness of this very recently evolved virus is astonishing; it’s adaptation to a wide swath of the animal kingdom including many mammals, and its close proximity to humans is highly concerning.
http://www.nejm.org/doi/full/10.1056/NEJMc2405937
A CANDIDATE FOR THE UNDECIDED
That’s it for a short update in the world of infectious disease. Next week to catch up, maybe we will discuss Oropouche virus, and why you might want to avoid travel to the Caribbean if you are pregnant, enterovirus D68 which causes a polio like paralytic disease in children, or the listeria lurking in your deli meat. Perhaps we will visit Dr. Jay Varma, Andrew Cuomo’s head COVID advisor, and his video-tapped bragging about attending dances and “sex parties” during the early COVID lockdowns in NYC, which he orchestrated—while regular New Yorkers had their businesses ruined and were prosecuted for opening restaurants and gyms, even with masks. Too bad he left NYC government after Cuomo’s unceremonious exit—Jay might have fit in well with Eric Adam’s administration.