

The Viral Season Hits Hard With the Youngest

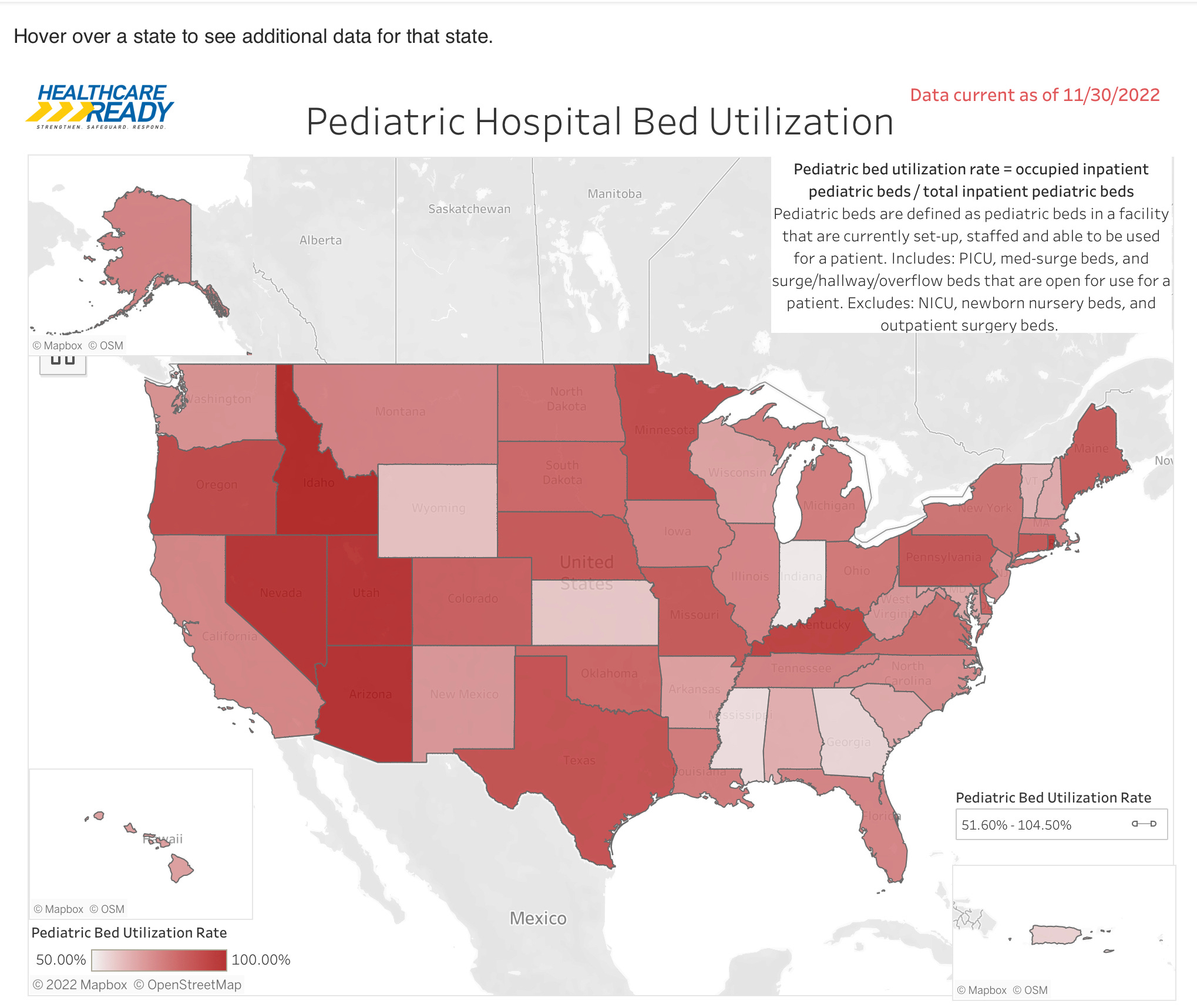
I started highlighting the unusually early and severe epidemic of respiratory viral illness in children 6 weeks ago, with a focus on RSV. The situation has only worsened with the arrival of Influenza now on top of continued high level RSV activity. CDC data shows RSV infections are 10 times higher than the historic average, and 171 out of every 100,000 infants under 6 mo of age were hospitalized for RSV in the week ending Nov. 12th. Compared to the pre-pandemic year of 2018, that is a sevenfold increase. Influenza activity is high across the country now, and continuing to increase week over week. The CDC is reporting 78,000 hospitalizations for Flu and 4,500 deaths so far this year (14 of them children) and a cumulative hospitalization rate for this week #47 which is higher than any season since 2010-2011. The pediatric hospital and healthcare system has been under pressure for 6 weeks or more, and the above map (as of Nov.31st) shows pediatric hospital bed occupancy. The dark red indicates near or 100% occupancy. With Influenza levels continuing to increase, and the likelihood that in addition to facility bed shortages we will likely see an increase in healthcare staff illness—the situation looks quite bad. At least four hospitals in Oregon, including OHSU which provides 50% of the state’s pediatric beds, have gone to crises standards of care. Multiple pediatric groups, including the Children’s Hospital Association and the American Academy of Pediatrics, sent letters to the White House and HSS on November 15th requesting that they declare a state of emergency, allowing all sorts of Federal support including military staffing—but so far the Biden administration has balked at that. I suppose crises is in the eye of the beholder, whether it’s an epidemic of pediatric disease, rioters or a southern border.
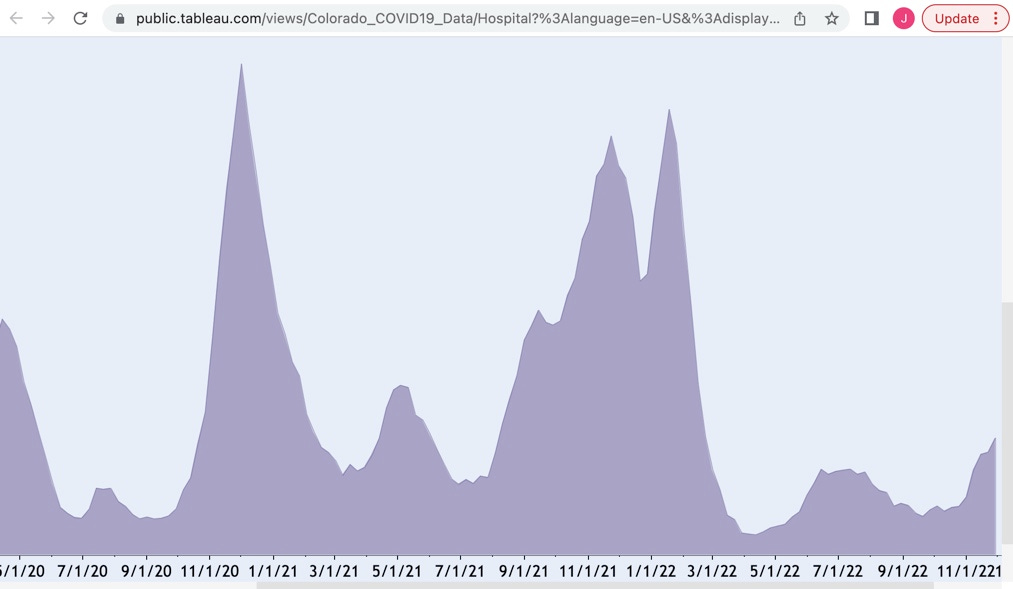
Switching gears to another respiratory illness, COVID, we find that hospital admission trends are increasing for the country as a whole. Below is a graph of Colorado’s COVID hospitalizations throughout the Pandemic. You can see that the current spike has surpassed the early summer surge of cases that was due to BA.4/.5, but is nowhere near what we experienced with the arrival of Omicron BA.1 in early January.
I think it’s safe to speculate that despite the current crop of immune escaping variants, the current winter surge will lead to far fewer episodes of severe and critical disease than BA.1/BA.2. Most of us have enough broad based B and T cell immunity through vaccines and infection with a variety of the Omicron clan to attenuate the severity of disease, even if that immunity won’t prevent repeated episodes of infection. Most, of course, is not all—and we have reached the point in the Pandemic where the disease is lethal, or severe enough to require hospitalization, essentially only in the over 65 yo age group, and the significantly immunocompromised. In fact 8 out of 10 people dying from COVID in 2022 were over 65. COVID was from the beginning a disease that weighed disproportionately on the elderly, but over time that difference has become even more pronounced; as the accumulated immunity has provided the younger members of the herd with enough protection to survive the virus’ widespread insults to various organ systems. Those of us starting with the various deficits attributable to age and pre-existing disease don’t fare as well. We even have the admission now from multiple media sources that the majority of people dying currently from COVID are vaccinated or vaccinated plus boosted. Why should that be the case? It’s simply a question of numbers. The vast majority of people in the older age group are vaccinated and many boosted. The vaccines and boosters confer a relative, but not absolute risk reduction, and there are just so few elderly left around who aren’t either vaccinated, or with immunity from a prior episode of COVID, that there’s little competition for the morgue. In early 2021, when cases of serious disease vaccine breakthrough began to be reported, I said (to the consternation of some friends who wondered if I might be an anti-vaxxer), “When everyone is vaccinated, the only people getting sick and dying will be the vaccinated”. No one should be fooled by these headlines into doubting the value of the vaccines and boosters in significantly reducing your risk of severe outcome. Unfortunately penetration of boosters in the at risk older population continues to be low (32.6%), and miscommunication from the government continues apace. We have previously discussed the repeated failures of the CDC in this realm. This week we were treated to dueling Tweets from Xavier Becerra, the Secretary of HSS, telling us to go get a booster if it’s been 2 months since your last booster; and Kamala Harris informing us that “Just one COVID shot every year is all most people need”. I’m not sure what science she is following, but given her poll numbers it’s possible she is angling for a change in portfolio, perhaps a shot at taking over Fauci’s job. As far as the 2 months between doses goes, I’m well aware of the CDC recommendations, and well aware of what scientific data to date tells us.
I have generally steered clear of the issue of Long COVID, other than to say it is difficult to develop meaningful data on a phenomena which is very subjective, and both hard to define and reliably measure. My take has been that it will fall into the categories of: Damage Done, Autoimmune or other Immune Activation, as a result of some persistent viral presence, or a manifestation of psychologic predisposition or Mental Illness. Also it’s my previously expressed belief that it will spawn a cottage industry of both genuine, academic inquiry, as well as the predictable quackery—that will prove highly attractive to the unhappy sufferers to the tune of many billions per year, with little to show for the investment. This is almost guaranteed to be the case since the Department of HSS issued guidelines qualifying Long COVID as a disability under the ADA act. There are 12 qualifying complaints listed, only one of which is remotely quantifiable through actual measurement. The retraction rate of peer reviewed, published articles on COVID exceeds that of similar articles published during prior time frames, and that includes papers on Long COVID. A recent study in JAMA Network Open reported that among a cohort of people who had respiratory illness during the Pandemic and reported prolonged symptoms considered typical of Long COVID, more of them tested negative for COVID during the initial illness than tested positive. Another finding was a very high detection of what the authors describe as “poor mental health” among both groups (22 and 27%). There are certainly issues that can be cited with the methodology and potential confounders, and as always I suggest you evaluate the findings for yourself if interested. Am I destined to be identified as a Long COVID denier, wear the dunce cap and publicly confess my sins? I hope not since I don’t pretend to have answers on this issue, but like any honest deckhand, I feel compelled to point out that the “cloud bank” everyone is reporting to the captain just might be an iceberg.
Association of Initial SARS-CoV-2 Test Positivity With Patient-Reported Well-being 3 Months After a Symptomatic Illness
JAMA Netw Open. 2022;5(12):e2244486. doi:10.1001/jamanetworkopen.2022.44486
That’s it for this week’s Infectious Disease review. In closing I’d like to reinforce that we are in an enormously better position than we were in the previous winter of the Pandemic that continues. In this season of Christmas, Hanukkah and Kwanza I’m leaving you with the following image that embodies the spirit of hopeful optimism in the face of persistent severe adversity. This was the first Christmas Tree erected at the site of the nascent Rockefeller Plaza. At the height of the Great Depression the workers chipped in for the tree and decorated it with handmade garlands, ornaments and strings of cranberries, made by their families.

Wondering if you could apply your amazing powers of analysis to why some people don’t get covid at all apparently, is it blood type? Luck? Not true and we all have had asymptomatic disease? Thanks!
Another excellent post! Thank you very much.