

The Waiting Game
“The waiting is the hardest part”

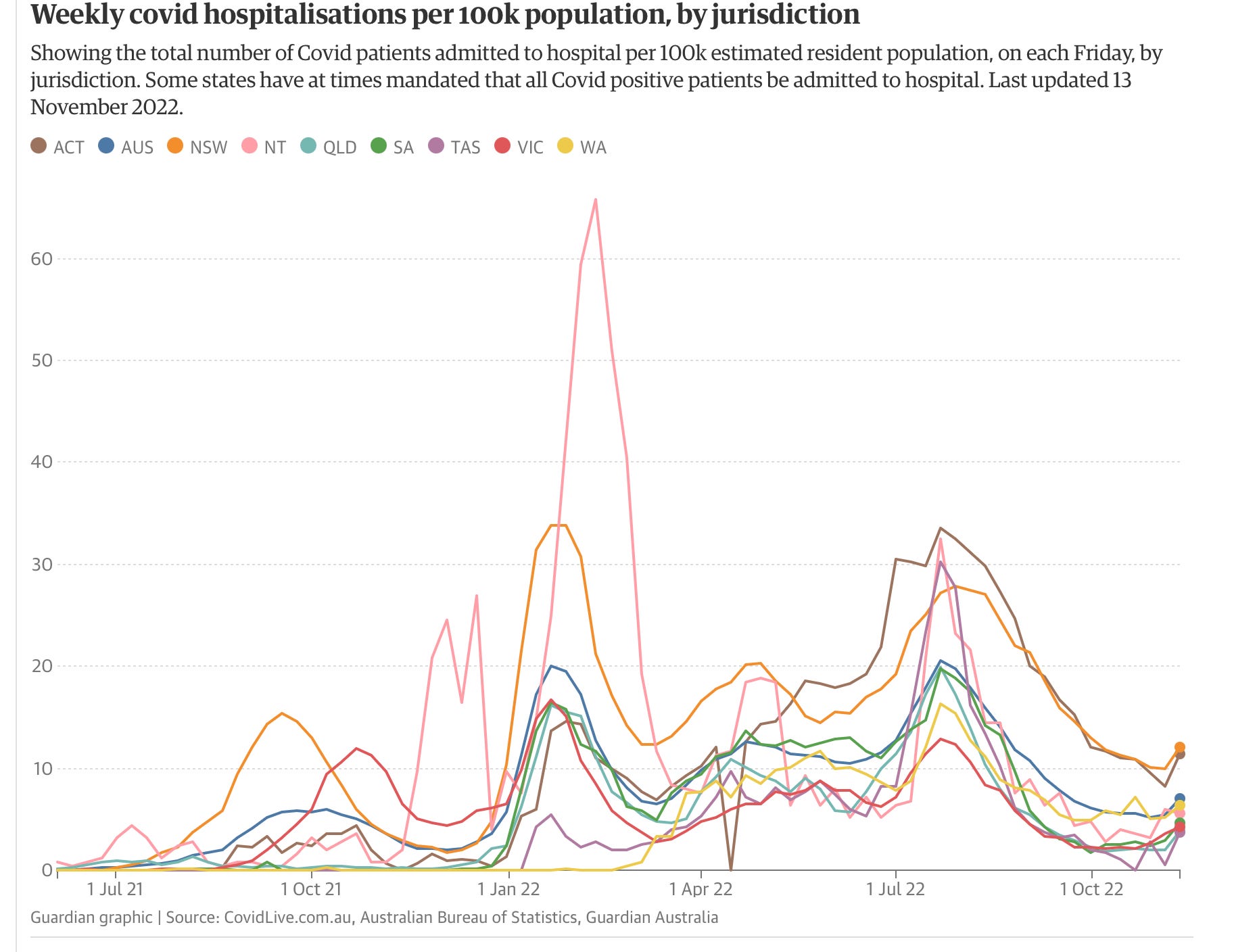
We are in the midst of the waiting game now, fairly confident that the winter surge will be much less traumatic than last year, but still with uncertainty about the impact of the new variants. They are going to escape much of the immunity built up from vaccinations, boosting and infection with prior variants, leading to some surge in cases. Japan is currently experiencing a major increase of COVID infections, reaching 100,000/day this week. Health authorities there are calling it an Eighth Wave. The Chinese are in the midst of a COVID explosion with 40,000 cases reported yesterday. This looks like it will surpass last year’s mid-winter surge, and the government of Guangzhou is racing to build 250,000 quarantine beds, as well as their signature hospitals which appear in 10 days. Chinese citizens are chaffing under the central government’s draconian NO-COVID policies, and the unthinkable occurred there this week—protest riots. There is a lot at stake in China. Despite their overall high vaccination rate, 50% of the population over 80 remains unvaccinated. The remainder of the population were vaccinated with the home grown Chinese inactivated viral vaccines, which have proven inferior to the mRNA vaccines. Australia is also recording both an increase in infections, and a sudden nationwide uptick in hospitalizations, as evident in the following graph. The spectacle of a Carnival cruise ship docking Monday in Sydney with 800 active COVID cases out of 4600 passengers is not a solid advertisement for the return of the cruise industry just yet, and likely to revive memes of floating Petri dishes. “For dinner this evening Madam, we are serving Norovirus, Flu or COVID—with boosters available in the purser’s office”.
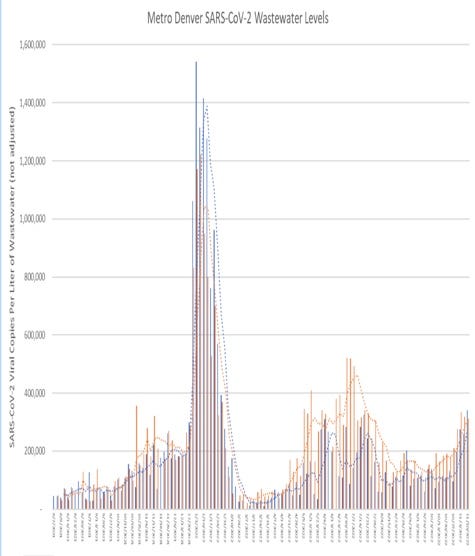
The data from Europe however, remains hopeful that we will continue to see an uncoupling of infection from severe disease and death. COVID burden currently is quite variable around the United States. The South and Southeast are in the midst of a large Influenza epidemic, but with relatively less COVID compared to other areas. Here is a look at my state of Colorado. As usual the waste water signal doesn’t lie, with a recent sharp increase in SARS2 in the metro area. (graph courtesy of my colleague Greg Craig)
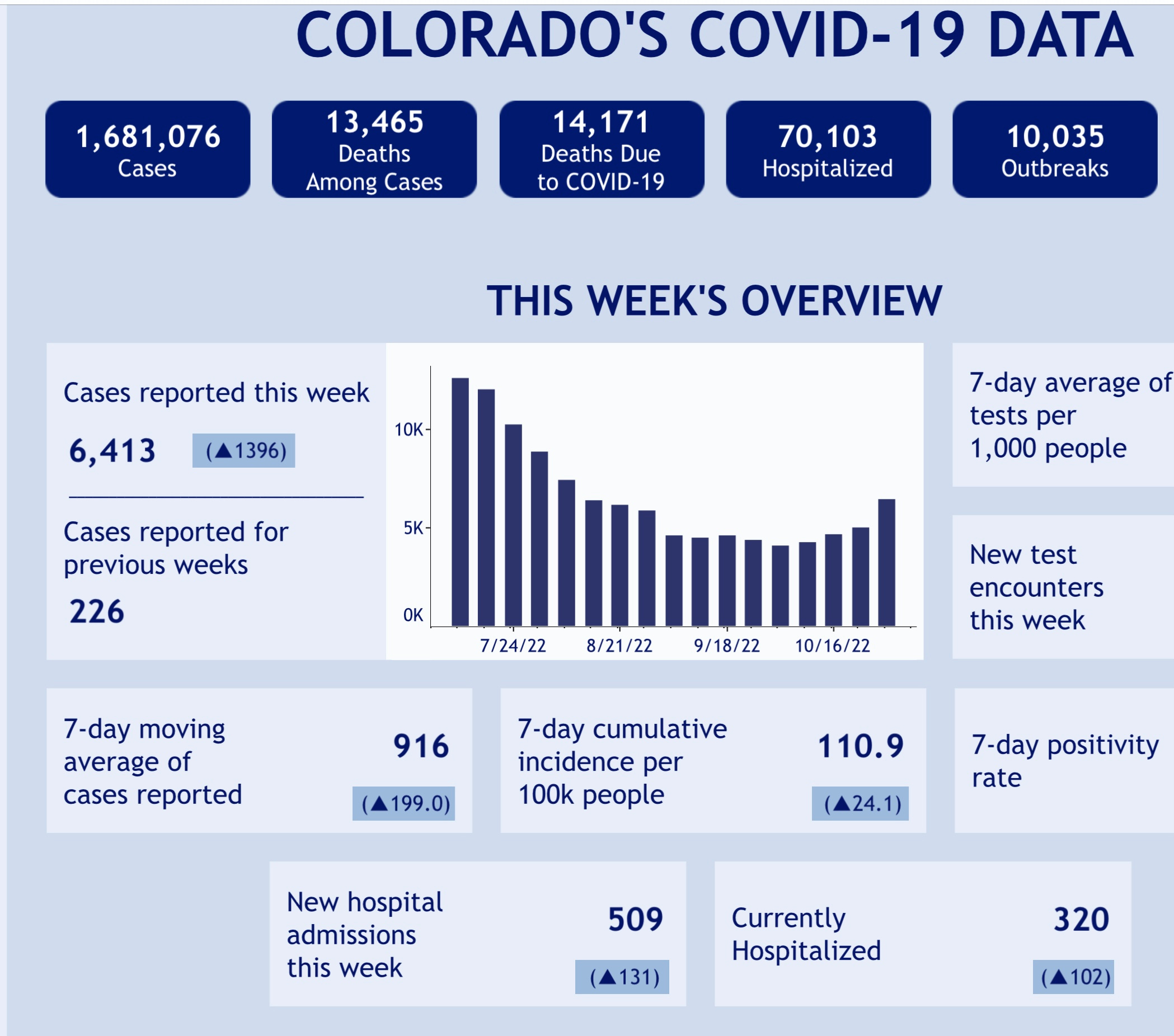
On this page, from the Colorado Department of Health, you can see that despite the very low levels of clinical testing, case numbers are rising, (as predicted by the poop) with a significant increase week over week since a low at the beginning of October. New hospital admissions have risen as well.
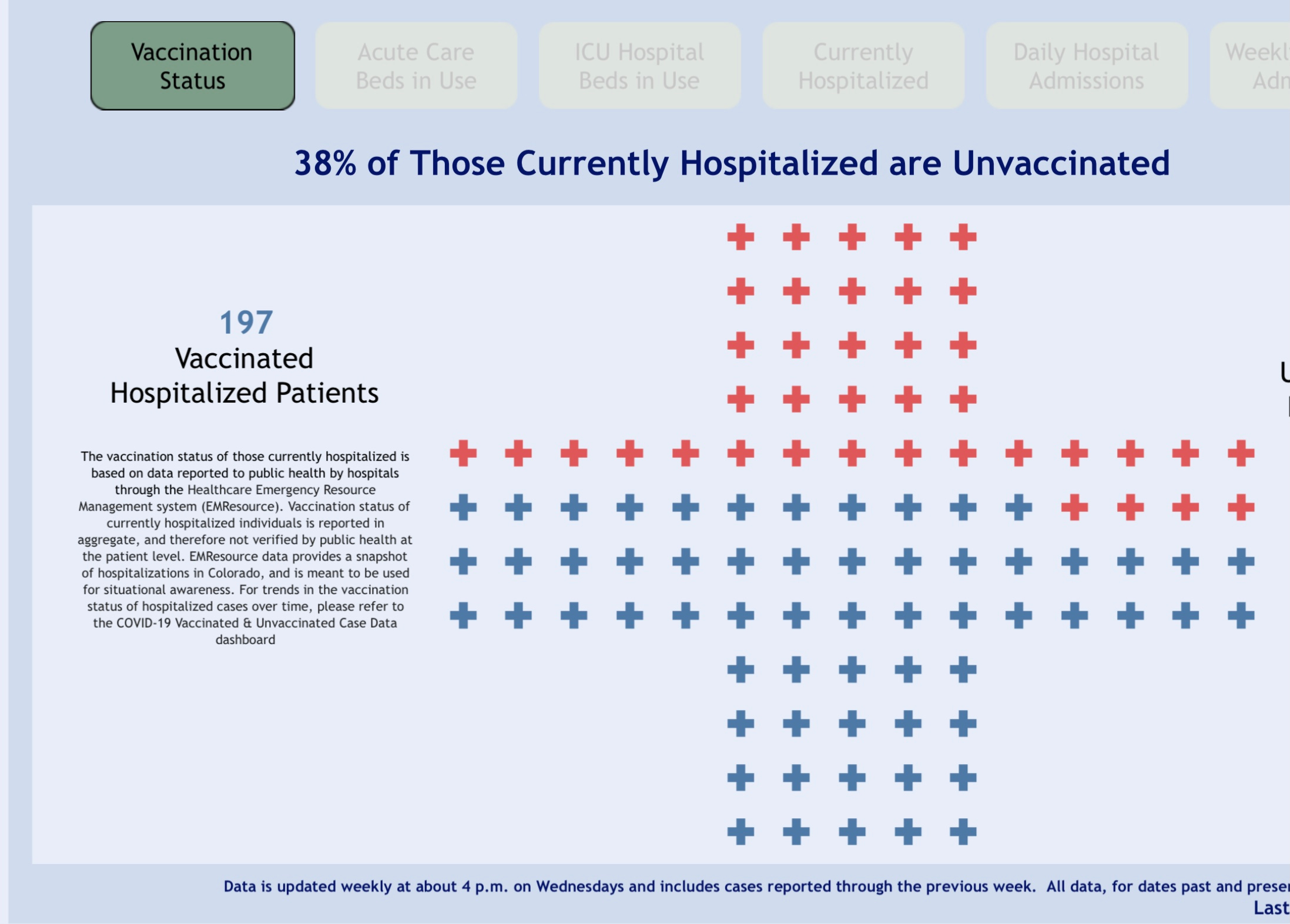
Two weeks ago (Connecting the Dots) I reviewed the CDC study looking at vaccine protection from severe COVID leading to hospitalization. I was surprised by the finding that in the BA.5 era protection from a booster had fallen to 30% by 3 months. Bringing it closer to home, I wondered what Colorado’s data would say about this. Here is the most recent state update on currently hospitalized COVID patients, showing that 62% are fully vaccinated, and 38% are unvaccinated. The data doesn’t tell us anything about boosters or timing from last vaccine dose, so admittedly it’s not very granular. Given that 28% of the Colorado’s population remains unvaccinated (62% vaccinated), my crude calculations lead to a vaccine efficacy in preventing hospitalization of 36%—not far off the number calculated in the CDC paper. Any statisticians out there feel free to chime in or correct me. Remember when the vaccines were first released, the data indicated that you were between 11 and 16 TIMES less likely to have severe disease? Two factors have dramatically changed: the appearance of the Omicron variants, which have significant escape from the original vaccine, and the fact that the vast majority of unvaccinated people have previously been infected (some with an Omicron variant). Between the unvaccinated having a sizable degree of natural immunity, and a vaccine poorly matched to the current circulating variants—and that match rapidly becoming more divergent—the booster efficacy a few months out from administration has unfortunately declined. The fact remains however, that if you are a higher risk person, you will have increased severe outcome protection in the range of 60% for several months after boosting. I suspect many of the most ardent vaccine cheerleaders have had to abandon the mantra, “this is an epidemic of the unvaccinated”.
There is a positive development on the therapeutic front with the FDA granting an EUA for the use of an existing drug Anakinra. This is a medication which blocks the action of two powerful inflammatory cytokines, interleukins 1a and 1b. These molecules are released early in the cascade of severe inflammation, that ends with some people in acute respiratory failure and ventilator dependent. In a RCT (randomized controlled trial) this drug, when given to patients with COVID pneumonia at high risk for worsening, both reduced the number of people progressing to respiratory failure, and at days 30 and 60, reduced mortality by about 45% (5.3% Anakinra and 9.7% placebo). Despite the current loss of effective monoclonal antibodies due to the newer Omicron variants, we do have substantial impactful therapy for severe COVID in the form of antivirals and anti-inflammatory medications.
Several recent articles have drawn attention to how the loss of effective monoclonal antibody drugs, due to viral mutation, is weighing heavily on the safety of people with compromised immune systems. {Katherine Wu, “The End of Evusheld”, The Atlantic} Hopefully new monoclonals with high level variant activity will be forthcoming soon from Regeneron, Lilly or other pharmaceutical companies. Their drugs were a major advance in treating COVID and saving lives, receiving FDA go ahead in November 2020, before we had vaccines. Monoclonal antibody therapy remains critical for the well being of huge numbers of people with immunodeficiency who are unable to mount a normal response to vaccine. They are also an important option for high risk people who have contraindications to oral anti-viral drugs. Given the torrid pace of COVID mutations, there is tremendous difficulty in developing these drugs and getting them out to the people in need in time to still be effective. The FDA could assist here by streamlining the approval process for this class of therapeutics. After all the FDA did just approve a vaccine based on the results in a few unhappy mice.
I get asked frequently by people just diagnosed with COVID whether they should take Paxlovid. There is significant reluctance by some physicians and pharmacists around the US to prescribe what I believe, is a very useful medication. The main objections are: an anecdotal perception that rebound of viral load and symptoms is a very frequent occurrence, and the fact that there are quite a number of drug interactions. Those drug interactions will require some thoughtful input from the prescriber, but in many cases other drugs can be temporarily stopped, or dose reduced without risk. This all boils down to the confidence level and knowledge of the prescriber, and the willingness to invest some extra time. In the main EPIC trial of Paxlovid (which demonstrated it’s impressive 89% reduction in mortality) the virologic rebound rate was 2.3% for Paxlovid versus 1.7% for placebo. The argument has been made that we are now in a different era, with Omicron variants and a mostly vaccinated population, and that rebound seems anecdotally to be MUCH more common than what was observed in the EPIC trial of unvaccinated people. In his November 16th “Ground Truths”, Eric Topol presents data from an (? as yet unpublished) RCT investigating the current frequency of Paxlovid rebound compared to no antiviral treatment. 95% of the participants were vaccinated and the trial was all run during the Omicron era. Their findings were an excess of 5% higher viral rebound, and 11% higher symptom rebound in the Paxlovid group. So why on earth would I say I continue to believe Paxlovid is a valuable therapeutic option? It comes down to the proven efficacy of the drug in lessening progression to severe disease and mortality. Patients having symptom rebound after Paxlovid are not experiencing severe disease, but mostly mild URI complaints. (I’ll take the runny nose over the benediction any day). The drug is not for everyone—it should be taken by people at high risk of severe disease, by dint of age, comorbidities or immune incompetence. Unfortunately, many prescriptions have gone to younger people who don’t fall into those groups; and the people who would benefit most are often denied treatment, because of concern for drug interactions, or the perception that rebound is much more prevalent than is actually the case.
A further reason to consider Paxlovid is it’s demonstrated efficacy in reducing Long COVID symptoms. The following is a link to the relevant Veterans Administration BioRx preprint and a quote from their abstract.
https://www.medrxiv.org/content/10.1101/2022.11.03.22281783v1
Nirmatrelvir (Paxlovid) was also associated with reduced risk of post-acute death (HR 0.52 (0.35, 0.77), ARR 0.28 (0.14, 0.41)), and post-acute hospitalization (HR 0.70 (0.61, 0.80), ARR 1.09 (0.72, 1.46)). Nirmatrelvir was associated with reduced risk of PASC (Long COVID symptoms) in people who were unvaccinated, vaccinated, and boosted, and in people with primary SARS-CoV-2 infection and reinfection. In sum, our results show that in people with SARS-CoV-2 infection who had at least 1 risk factor for progression to severe COVID-19 illness, treatment with nirmatrelvir within 5 days of a positive SARS-CoV-2 test was associated with reduced risk of PASC regardless of vaccination status and history of prior infection
That’s it for you weekly ID and Pandemic briefing. Brought to you from the Banana Republic where we are still in a waiting game to know who our elected Congress person is nine days after election night. Rumor has it that Colorado and other states may bring in Big Bird to assist with the counting. I suppose it may just reflect the national set back in Math skills discovered after our Pandemic Education Experiment. I might not report an update next week, given the high likelihood that there will be rampant tryptophan/football coma, or the marginally less likely prospect of nuclear war by then. Thanks for your time and interest. Please continue to direct your friends here for quick updates and analysis. Comments are always welcome.