

The World According to COVID
Variant Porn, Surges in Europe and Asia, Vaccine 4th Doses and CDC Data

Several articles have appeared recently recycling the Deltacron story, and I have been asked about its significance. Aside from some more recent evidence that this is actually a recombinant virus, made from long genetic sequences of the Delta and Omicron variants, and not a laboratory contamination issue, there is nothing to suggest that Deltacron is the new bad boy. Certainly the basic description of this recombinant was concerning; plug the Omicron spike, which made that variant so highly infectious, onto the rest of the Delta virus, which was more virulent, and you might have had a serious contender for the next very bad variant. But passage of a short time has shown that Deltacron has remained a very rare sequence, and has not competed successfully against the various Omicron lineages dominating the world now. That may have simply been a matter of timing. Deltacron was late to a party where Omicron had already danced with so many, that it hit a wall of effective immunity. Most likely we will never know. I’m not sure what spiked the resurgence of interest in Deltacron, other than the need to publish some variant porn and compete against the War for the reader’s attention. Significant concern should remain focused of BA.2 which is overtaking the original Omicron right on schedule.
As highlighted in last week’s post there is a large surge in COVID occurring in the UK, northern and eastern Europe. Not just cases, but hospitalizations, are increasing again in multiple countries. The reasons for this are unknown and everyone has an opinion. I don’t think it’s going very far out on a limb to assume that BA.2 is a significant contributing factor, along with relaxation of various mitigation efforts. A consistent pattern throughout the pandemic has been a surge of disease in the US following a surge in the UK and Europe by just a few weeks. After the relatively small Alpha wave here, I started calling England the “canary in the coal mine”, and the Delta and Omicron surges bore that out. For an in depth look at the opposing arguments for and against this pattern holding up, and presaging another wave of US disease, I refer you to Eric Topol on Wednesday in The Guardian, “Once again America is in denial about signs of a fresh COVID wave”, and Rachel Gutman in the Atlantic on Thursday 3/17, who quotes a number of experts pointing out reasons why this may not be the case. Since I’m an aficionado of divining the waste water data, I’m going with Eric Topol’s assessment, given that the recent 3/10 CDC update on waste water showed that 15% of 410 locations sampled around the US registered a 1000% increase in COVID levels compared to the prior 2 weeks. Now it’s possible that much of this increase in disease is very mild or asymptomatic, and that reduced clinical testing is leading to an undercount of cases. If that’s true, it is just one more marker along the road to COVID becoming an annual endemic disease.
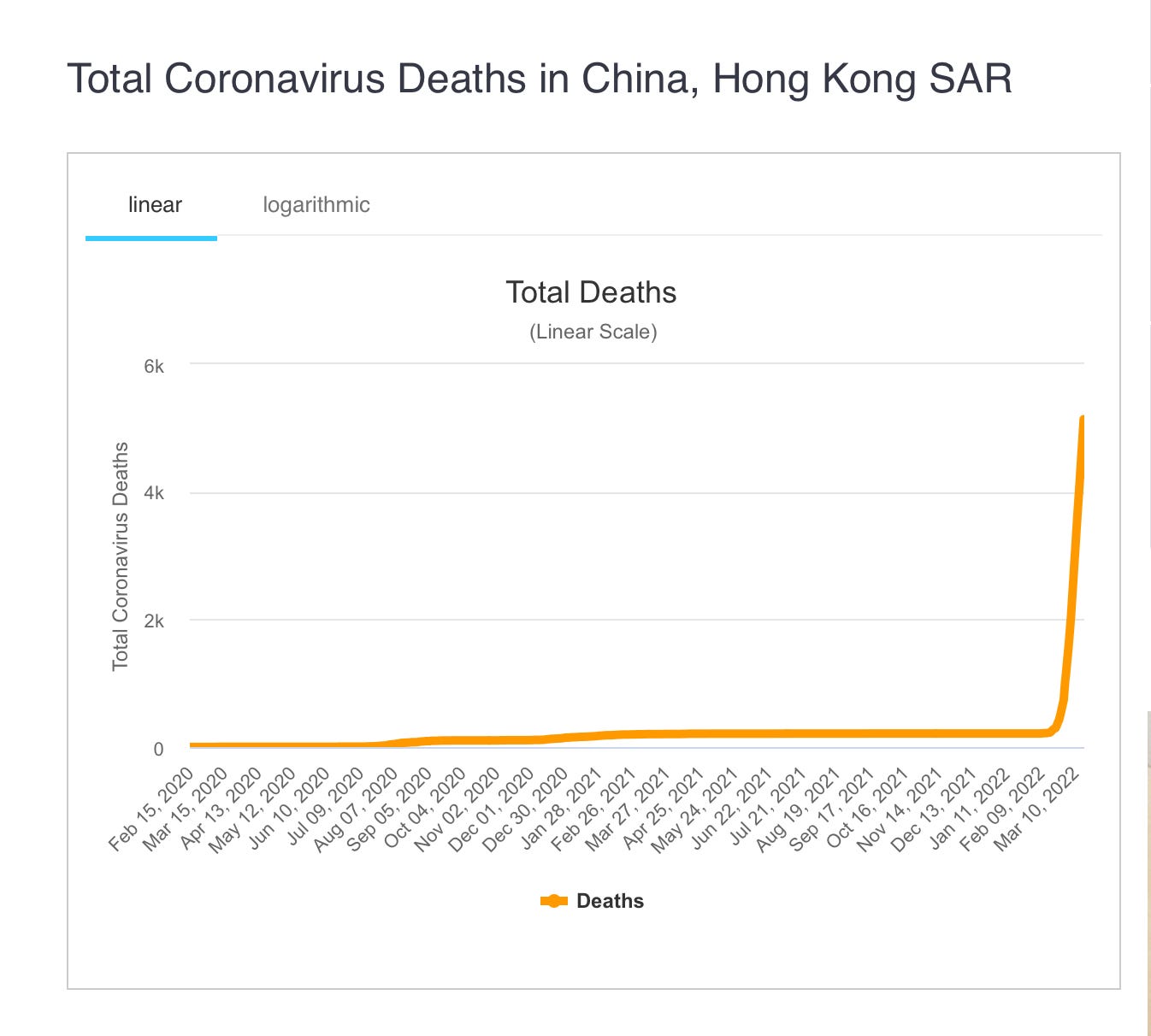
For a dramatic illustration of what happens when Omicron enters a population with no prior immunity from other variant waves, and only vaccine induced immunity in a portion of the population, I’m including the following graph of the Hong Kong death rate from COVID throughout the pandemic. Omicron, which the media assured us prematurely was very mild, is a very effective killer when up against weak and nonspecific immunity.
As you probably know Pfizer and Moderna have asked the FDA to approve a 4th dose of vaccine. Pfizer apparently requested permission for the age 65 and up group, although it is not clear to me from comments of their CEO, Albert Bourla, whether they plan to ask for a wider indication. Not to be outdone and second in line again, Moderna has requested an indication for everyone over the age of 18. My reading of the data available so far is that a third dose was still significantly protective against severe disease and hospitalization during the Omicron wave. Even a recent booster was not highly protective against infection, and there is no good evidence that a fourth dose significantly increases that protection, at least for any reasonable amount of time. Similarly, there is not adequate data available to make a solid judgement on the duration of the good protection from severe disease conferred by the third shot. This, coupled with the rapidly declining disease rates around the country, lead me to conclude that this submission is premature. As you recall it was just 5 weeks ago that a request from Pfizer to approve the vaccine for the 6mo-4yr age group was tabled by the FDA pending further data proving effectiveness. No one should deny Pfizer and Moderna did an outstanding job delivering in record time a safe and effective vaccine that saved countless lives, but before we nominate them for Sainthood we should just consider that they are corporations driven by the profit motive. Sorry to dredge up dirty laundry from more than a decade ago, but Pfizer is the company that once paid the highest fine ever levied (to that date) against a pharma company, 2.3 billion dollars, for fraud, illegally marketing their pain killer Bextra for indications it had not been granted and for misrepresenting clinical trial results. They paid a further $400 million dollar settlement in 2015 for misleading investors about the same drug, which was withdrawn from the market with allegations that they hid certain adverse safety signals during the initial FDA approval.
Here is my advice in navigating this issue. Be triple vaccinated. If you were vaccinated and came down with Omicron I would not seek out further vaccination at this time, you have now been “vaccinated” with this year’s version of the virus. If you were triple vaccinated and significantly exposed to Omicron but didn’t become infected, I would not seek out further vaccination at this time. People who should consider a 4th dose of vaccine are those with moderate to severe immune compromising conditions, who are expected to mount a poor response to vaccine, or who have severe co-morbidities making the risk of death significantly higher from any serious respiratory infection. For the moderately or severely immune-compromised the antibody cocktail Evusheld is a much more effective option, but unfortunately remains extremely hard to find, with no accurate federal or state listings of sites where it can be obtained. Other triple vaccinated folks, without history of infection, should take a wait and see approach, carefully looking for renewed surges of COVID, new variants which might render the current vaccines even less effective, and the release of new data informing us about the duration of severe disease protection from the 3-shot regimen. Speak with your doctor, and let Albert Bourla talk to his investors and the FDA.
The last item I would like to cover is a continuation of the tale of the CDC’s terrible record of communication. This week the CDC Data Tracker’s tables of COVID death statistics suddenly and dramatically changed with an across the board 72,000 death reduction, and a notable 24% decrease in the number of child deaths since the beginning of the pandemic. This was accompanied only by a footnote stating changes were made due to adjustment for a “coding logic error”. This was immediately picked up by a number of people and reported on various social media outlets, but as far as I can tell was studiously ignored by the mainstream media. Now in a highly charged atmosphere you might expect the CDC to anticipate that removing 24% of pediatric deaths from their tally, without addressing it specifically, visibly, and in detail ahead of time (or at least in real time) would create the impression of trying to hide something and pull a fast one. But instead they opened themselves up to exactly those accusations and fed grist to the conspiracy mill for no good reason.