

The World Virome is Huge
How about your own personal Virome?

Viruses are the most numerous biologic entities on earth, and by Virome I am referring to the sum total of all those viruses. While there may be 9 billion humans, a single person with HIV infection for example, can have 10 billion new viral particles produced per day. Viruses infect all three cellular domains of life, the Bacteria, the Archaea (which resemble bacteria), and the Prokaryotes (all life forms whose cells have a defined nucleus). It’s estimated that the genetic diversity of viruses and bacteriophages (viruses that infect bacteria and archaea) is orders of magnitude greater than the genetic diversity of all the plants, animals, and unicellular prokaryotes. So far scientists have identified only a tiny fraction of viral genes, and the function of only a tiny subset of those. As we learned first hand during the COVID Pandemic, some viruses mutate extremely quickly, and in unpredictable, unforgiving ways. We can make highly informed, educated guesses about the most likely viruses to be the cause of the next human Pandemic, and in fact some virologists accurately predicted it would be another corona virus following the SARS1 outbreak 20 years ago. That was a lucky guess informed by extensive knowledge, good reasoning and intuition—but still a lucky guess. We can speculate that the next pandemic will be some iteration of Avian Influenza; perhaps even the H5N1 currently decimating birds, and moving into an ever expanding circle of mammalian species, or another bat corona virus via some intermediate host. I’d be willing to bet that the debacle of the last three years might not be enough for some Chinese to abandon their taste for a good civit cat stir fry, a nice pangolin confit, or raccoon dog roast.
Even with our ability to make logical assumptions about the most likely viral pathogens with pandemic potential, there is the distinct possibility of another black swan event. This Pandemic may have conditioned some of you to think, well if that happens we will have the mRNA technology to whip up a vaccine on Tuesday and get it into arms by the next Monday. That might be true for some types of viruses where we have a pretty good understanding of their functioning, and a good immunogenic target to block infection, but massive efforts over forty years to develop an effective HIV vaccine have failed. Let’s also not loose sight of the fact that despite the incredibly quick isolation of the SARS2–Cov19 virus, the immediate sequencing of its genome and the most rapid vaccine development in history, there were still an official 7 million deaths, and more likely 20 million, world wide. Scientists can and should make all the predictions possible based on multiple sources of data, but nobody saw the HIV pandemic coming, possibly resulting from a single transfer event of a Chimpanzee virus to a human hunter. The HIV pandemic has unfolded like a train wreck in slow motion over 42 years; and while the dramatic and very painful early years prior to effective treatment may be fading from most people’s memory, the following statistics should serve as proof that we cannot ignore the possibility of a completely unexpected event dished up by the enormous world wide Virome.
Global HIV statistics
38.4 million [33.9 million–43.8 million] people globally were living with HIV in 2021.
1.5 million [1.1 million–2.0 million] people became newly infected with HIV in 2021.
650 000 [510 000–860 000] people died from AIDS-related illnesses in 2021.
28.7 million people were accessing antiretroviral therapy in 2021.
84.2 million [64.0 million–113.0 million] people have become infected with HIV since the start of the epidemic.
40.1 million people have died from AIDS related disease since the start of the pandemic.
If we accept that an unpredictable pandemic event is possible, then the logical conclusion is that world governments need to concentrate on surveillance and the infrastructure for rapid response and isolation. That should take precedence over investing enormous resources into trying to predict the next big thing. It’s great to have a giant stockpile of Avian Influenza vaccine, as our government has acquired, until you find out that the pandemic Avian Influenza strain that shows up is so far genetically removed from your prior best guess, that you may as well be burning incense to ward off the ‘bad air’. Waste water metagenomic analysis will be a crucial element added to our more traditional surveillance techniques. The technology has grown rapidly during the COVID Pandemic, and proven that it not only accurately reflects the amount of viral disease present in a community in real time, but also detects the introduction of new variants. Variant identification during COVID was generally based on using probes for known genetic signatures of different strains of the virus. Going forward, looking for an unknown pathogen that might be the next bad boy, metagenomic analysis of waste water has great promise. Instead of looking for some predetermined pathogens which the scientists have predicted as the most likely culprits to appear, all of the genetic material present, both DNA and RNA, are completely sequenced. All the bits and pieces, from small snippets to full genomes are then compared to the full library of all known viral and bacterial sequences. This is possible through the use of computer programs and AI comparing enormous numbers of possibilities very quickly. It may reveal the sudden appearance of a known virus that wasn’t expected as the cause of an outbreak, or something completely novel. If some brand new pathogen shows up, chances are excellent that it’s related to some previously catalogued viruses, and we have a good start in understanding the threat.
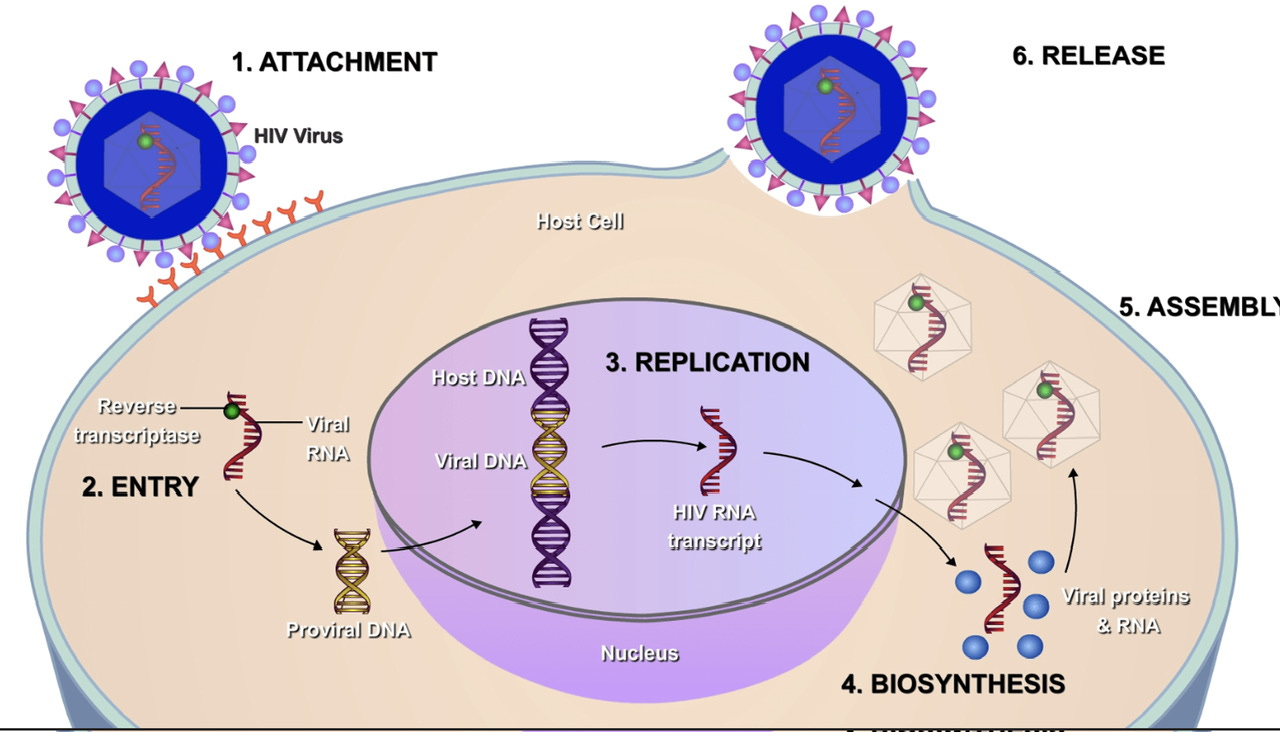
Let’s shift now to our own personal Virome, and how this intersects with the problem of Long COVID. Science has provided us with the knowledge that many viruses persist in the human body for very long periods after the acute infection has resolved, and in some cases for life. HIV, Hepatitis B and C, Varicella Zoster, Herpes Simplex and other Herpes viruses, HPV, CMV, Epstein Barr Virus, and Measles and JC Virus in some people, are among the most well known; but there are others, both known and unknown. On the particularly disturbing end of the spectrum is Ebola, which can routinely persist in immunologically sequestered sites like the testes for months after all signs of illness are resolved, and has been known to relapse up to 5 years later. In fact there is a great deal of viral baggage in our genome which has nothing to do with viruses we have personally been infected with. These viral sequences make up 6-8% of human DNA, and are the result of very ancient epidemics in our ancestors caused by a particular class of pathogens called retroviruses. HIV is the best known modern retrovirus to have caused a pandemic, but the record of our chromosomes shows with certainty there were many others. Much of this genetic material appears to be silent now, but some genes are transcribed and produce viral proteins—perhaps we should call them human proteins since we have been in possession of them for millions of years. Below is a simplified diagram of the HIV retroviral life cycle showing how the virus intercalates a DNA copy of its RNA into our chromosome
Data has been accumulating over the past two years that SARS2-Cov19 can persist in the body long after the acute infection. Initially this was found in people dying from severe COVID, where virus was found at autopsy throughout multiple organs, later it was extended to primarily immunocompromised patients who failed to clear the infection for up to a year and more. More recent studies have demonstrated the persistence of viral RNA and proteins in people with Long COVID symptoms. These folks may have negative nasopharyngeal and serum PCR for the virus, but excrete virus in their stool or have positive tissue PCR. For an excellent bibliography of the published work on the subject, and a thoughtful discussion of how persistent viral infection may lead to the pathophysiologic underpinnings of Long COVID, I refer you to the following May 10th paper in Lancet Respiratory Medicine.
https://www.thelancet.com/journals/lanres/article/PIIS2213-2600(23)00142-X/fulltext
Association of SARS-CoV-2 infection and persistence with long COVID Chengliang Yang, et al.
This dovetails nicely with the line of evidence developed by Martin Schafer, Marc Johnson and collaborators, (discussed in my post of last week, “Sleuthing the Sludge”) that persistent cryptic COVID RNA sequences found around the country are likely the result of viral evolution in chronically infected people. Some subset of Long COVID patients appear to have continued long term persistence of the virus, and the inflammatory, and immunologic consequences of this. Perhaps there are other relatively asymptomatic people with a subtle immune defect which prevents them from clearing the virus. It will be interesting to see results of the ongoing NIH sponsored study looking at Paxlovid as a treatment for Long COVID, so far all we have are anecdotal reports of responses. These chronically infected people are unlikely to pose any significant risk of contagion (no COVID Mary situations), but they are potential incubators of new viral variants, and the law of big numbers is always on the side of the virus being able to hit upon a new combination of mutations with unpleasant consequences.
Finally we check in on the US COVID status. The Public Health Emergency ended yesterday—I hope the White House remembered to send the memo to the virus. As you have undoubtedly read various data sources used by the CDC will be sun setting, along with free testing, free vaccinations and many people’s Medicaid coverage. Hospitalizations and deaths continue their slow decrease with 5-6% fewer of both from the prior week period. Various XBB variants now comprise essentially all the circulating virus in the US. XBB.1.16, the variant we have focused on recently, is not coming on as strongly as I had expected, which is great news. The fact that it is not rapidly out competing XBB.1.5 suggests its ability to spread faster and avoid prior XBB immunity is fairly limited, and not likely to lead to any significant short term surge.
I was called out last week on my suggestion that I would like to lead the CDC, given my well known love of bureaucracy. The truth is I had my sights set on Rat Tzar and CDC was always a second choice. Looks like neither of those is in the cards, but I am available to look into other small problems like our Southern Border, some disagreements in Ukraine, and the pesky changes in climate. Thanks for passing these posts to your circle of friends and colleagues. I’m running a special this week—you will receive a personal engraved Thank You on Rat Tzar stationary for every new subscription.