Viral Creep
Fact Check: Zombi pigs spotted in Indonesia— FALSE

Two posts ago we discussed African Swine Fever among examples of nonhuman viruses with the potential to cause severe human problems and food insecurity. I mentioned this virus’ path across the globe and its current expansion into new areas of Indonesia. Right on schedule this week, the Indonesian government announced that the largest pig farm in the country, which exports 15% of the all the pork consumed in Singapore, has been decimated by ASF virus. This farm is located on uninhabited Bulan island, close to a larger populated island, and is surrounded by watch towers. The operators were not so much afraid of some local villager crossing the water and making off with one or two of the 200,000 porkers—they were afraid of the introduction of ASF, with contaminated human shoes, clothing or tools acting as the vector. Just as SARS2-COV19 found its way into every obscure human habitation from Inuit settlements, to small islands, to villages up the Amazon from Manaus Brazil, ASV virus has proven to be an intrepid traveler. Once on Bulan Island it quickly killed 35,000 pigs, and another 120,000 were culled since they had been exposed. That is an enormous number of tons of carcasses, which were hastily buried in huge trenches—with the stench sickening villagers across the water. In November of 2020 Denmark, culled 17 million COVID infected mink and disposed of them in a similar fashion, only to have some of the dead mink rise up out of the earth from the pressure of gas produced by the decay process. Swine are pretty heavy so I doubt there will be a similar spectacle of zombi pigs to enter Indonesian folklore.

. https://thebulletin.org/2022/08/frankenswine-no-but-research-on-zombie-pigs-raises-life-or-death-ethics-questions/
Let’s leave the animal world and discuss viruses that affect the species at the top of most peoples’ list. (Apologies to dog or cat lovers). A graphic I included in “Influenza A is Still Top Dog” on 4/14/22 depicted how that virus makes use of reassortment to produce rapid shifts in its genetic make up, much quicker than the process of individual base-pair mutations. Other viruses can similarly make wholesale swaps within their genome, and emerge overnight as something entirely different in the human disease realm. This appears to have happened in France during the past year with a virus named Echovirus-11. Most infections with this virus are mild, self-limiting, often GI infections. In the past it has been a rare cause of severe neonatal infections with sepsis. Since July of 2022 nine cases of severe neonatal sepsis, with multi-organ failure and seven deaths have occurred in France due to this virus. All of these cases were infected with a new recombinant lineage of Echovirus-11, not previously seen. This new Echo-11 is suddenly responsible for a significant increase in the number of viral neonatal sepsis cases with liver failure, and a mortality rate much higher than historically noted. The timing of the cases shortly after birth suggests transmission of a mild acute maternal infection to the neonates. The sad outcomes are the intersection of a “new” virus, probably with some increased virulence factors, babies with immune systems not yet readied to respond, and acute maternal infection just prior to delivery, with hence no antibody response to cross the placenta. Because of the nature of transmission this virus posses no threat of pandemic spread, but this new lineage appears to have rapidly replaced the older strains of Echo-11, and in the last two months represents all the sequences submitted to the databank GSAID. So far the population at risk appears limited to neonates, and especially premature infants, but we should not ignore the possibility of this virus becoming a significant “new” pathogen for immune-compromised people. Below is a link to a CIDRAP bulletin of 5/31 regarding this, and WHO report.
https://www.cidrap.umn.edu/enterovirus/france-reports-rise-severe-neonatal-infections-enterovirus-variant
If it seems like you are being inundated with news reports of viruses you never heard of, many doctors are in a different cabin on the same boat. Only a few years ago many episodes of disease (frequently respiratory illness) which seemed clinically to be infections, would prove to have no bacterial cause, and we doctors would decide it was an unknown virus. Certainly there were some major pathogenic viruses we could specifically diagnose (often with a long delay), and sometimes treat; but there were innumerable situations where we felt the disease was viral, however proof was lacking. Viruses are much harder to culture and require specialized laboratories not found in most hospitals. That all changed as highly specific molecular genetic testing with fully automated analyzers made their way from research labs into almost every commercial and hospital lab. Now a swab taken from the patient’s throat or nose is put into the analyzer and within a short time it spits out results for perhaps 20 different pathogens, both viral and bacterial. Immediately the patient has Human metapneumovirus, Parainflueza virus, Adeno, Echo, or Distemper virus (if your patient is a Pomeranian). The revolution caused by rapid molecular testing has exploded our knowledge of human infectious (and neoplastic) disease. Without this, and similar sequencing technology, we would have been completely in the dark about the succession of COVID variants that sped around the globe assaulting mankind for the last three and a half years. This is a shout out and acknowledgement of the Molecular Biologists whose research has led to this revolution in medical diagnostics. Regarding other members of that club, and some Virologists, who are convinced science can never advance unless they are allowed to dice and splice together new viruses with increased capacity to infect humans—maybe their parents should have slipped a copy of Aristotle’s or Kant’s Ethics into their childhood chemistry set.

As far as COVID is concerned, we know less than we used to about its ebb and flow. In the US, new hospitalizations continue on the slowly decreasing slope and are at 7000 last week, down about 8% from the prior week. COVID deaths are now reported as 1.5% of total deaths (CDC does not supply that total number) but for some reason that is a 7% increase from the prior week. That bears watching to see if it’s a statistical aberration. XBB 1.16 (Arcturus) and XBB 1.9.1 are displacing XBB 1.15–nothing remarkable about them, and at this point even I’m not paying attention unless some significant surge starts, driven by new variant not of this lineage. XBB is exploding in China as we discussed last week, and the Chinese government’s messaging to the public is squarely aimed at pretending nothing of significance is happening.
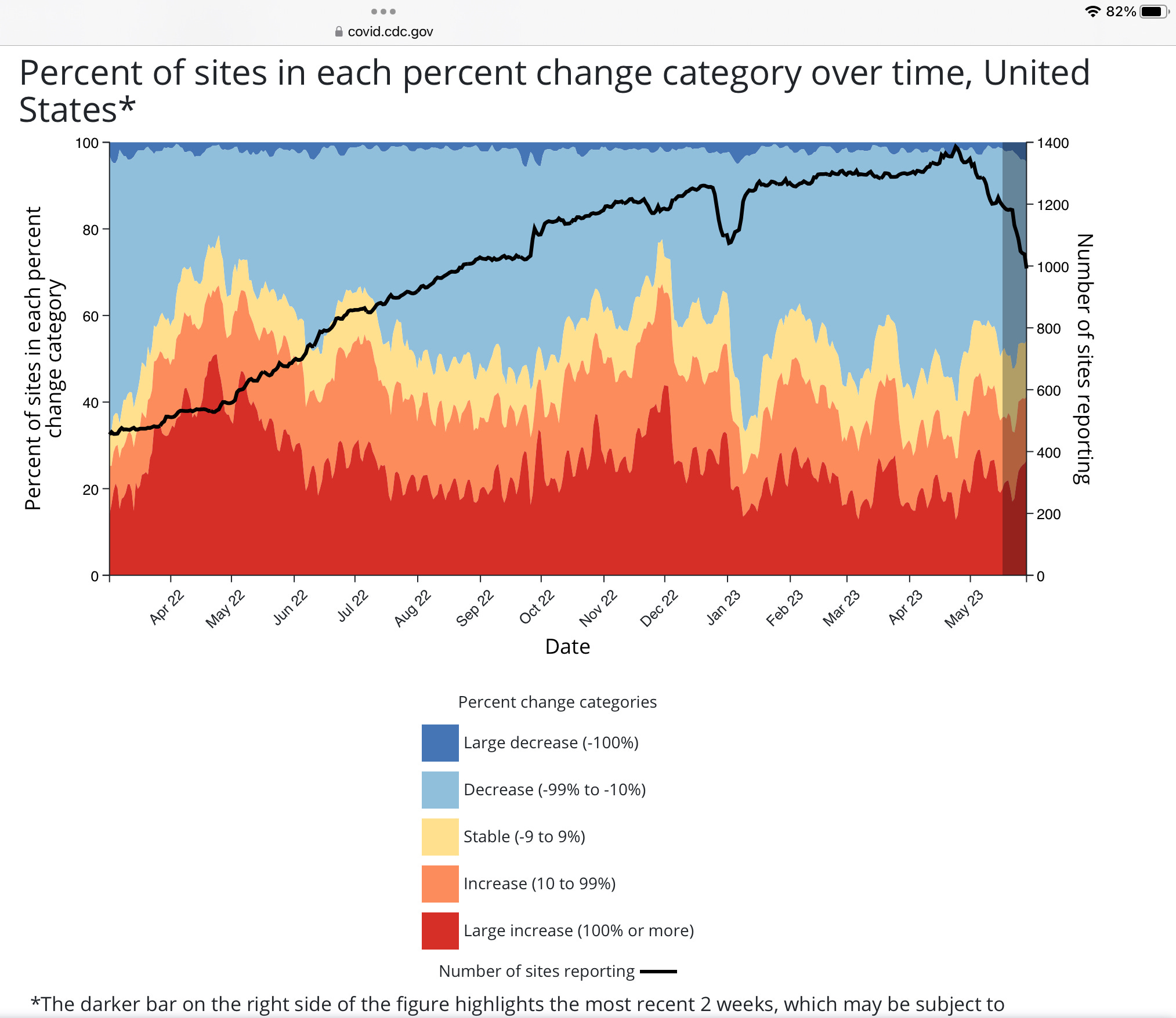
US waste water surveillance shows there is still plenty of COVID around, with continued marked differences around the country. The virus is sending fewer people to the hospital now due to: some reduction in severity of the Omicron lineages compared to earlier variants, accumulated natural and vaccine immunity, and perhaps the fact that it has already killed over 1.3 million, diminishing the supply of most vulnerable targets. For those readers who are not familiar, the following graphic shows sites reporting rapid COVID increases as red or orange and those with rapid decreases in blue. Unfortunately it doesn’t show us a measure of absolute viral numbers. (The black line shows the fall off in the number of sites which are continuing to do this monitoring).
The final comment today was submitted by the, “I Can’t Believe It’s True Department”. On Tuesday the communist paradise of North Korea was elevated by the WHO to be one of the ten member states on the Executive Board. At the same time Taiwan, a friendly democracy with one of the highest standards of Public Health in Asia, was not allowed to even attend the meeting for fear of enraging China. A few years ago a North Korean soldier managed to escape across the DMZ to South Korea, as I recall he had 10 active infections. This means that the psychopathic murdering lunatic Kim Jon Un, who oversees the starvation of his population, and routinely threatens nuclear war, will now get a vote on appointing WHO Regional Directors as well as the next Director General of WHO. The prestige and authority of the WHO is in a flat spin headed straight for the ground, where the pieces will land in China. This is at a time when the WHO is pushing for greater power over the actions of sovereign states during times of health emergencies. I hope we have learned that one size doesn’t fit all when it comes to incredibly complex situations like a pandemic, and I for one have no confidence in the WHO being the tailor.
Yesterday in Telluride it snowed enough to cover the trees. This May has been the wettest month in 10 years for Denver and the 11th wettest on record—good news for the state and others who depend on the Colorado river. Yesterday the White House announced their pick for the new CDC Director, let’s sincerely hope that is also good news for another agency which has seen its prestige and influence decline in recent years. I’m sure you can find a close friend or enemy to send these reports to, just remember to maintain plausible deniability of the source, in case they work for the WHO. The first button below will supply suggestions for any intrepid soul looking to better the state of the world. The second button is self explanatory and comments are appreciated. The final button links to some lost episodes of Mr. Roger’s Neighborhood.
Jeff- you’re a breath of sanity and fresh air in the current medico-political morass. A New Jersey gem!