

What Goes Around Comes Around
In Plagues, Life and Politics.

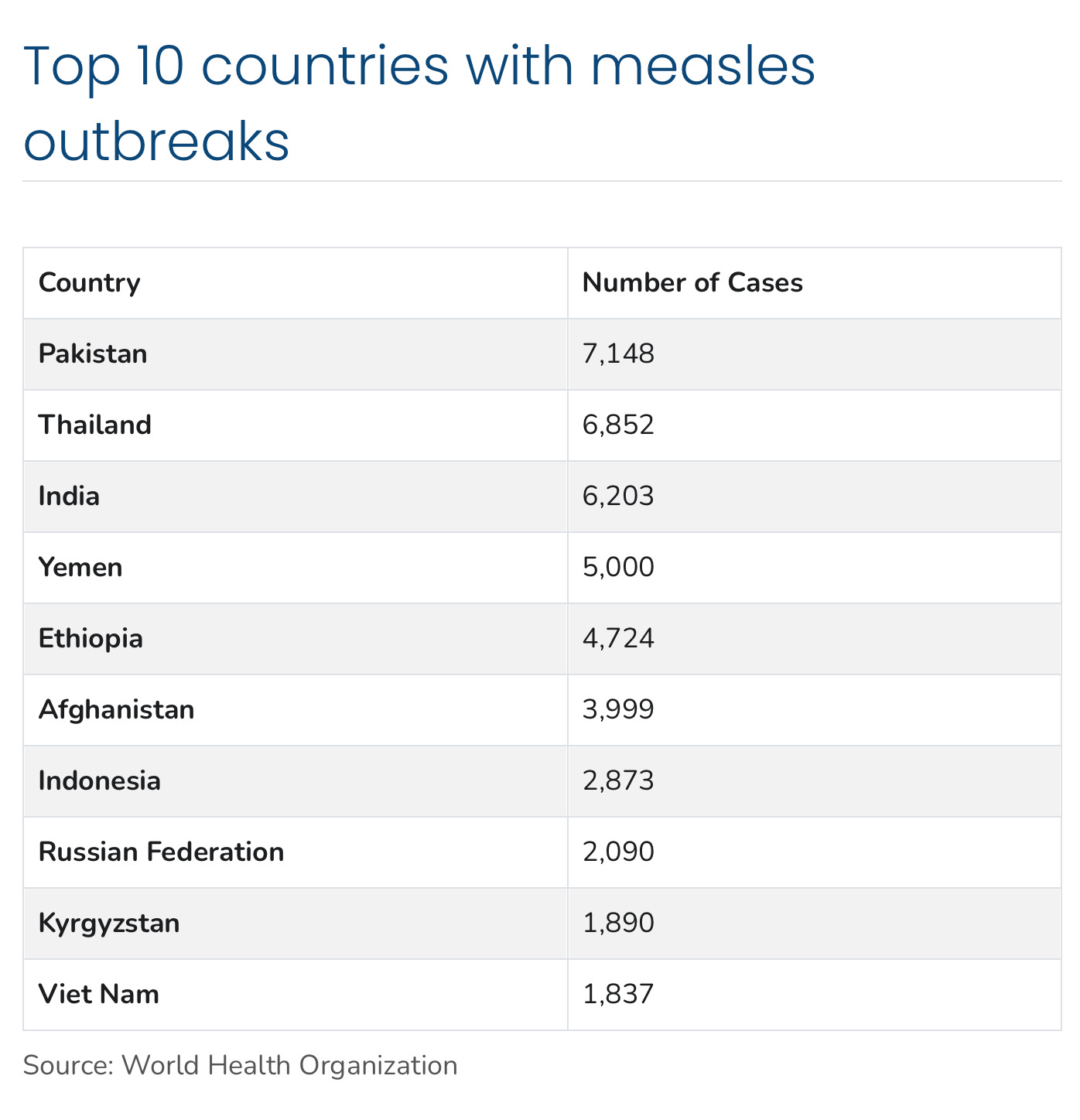
One year ago I published a post entitled “Measles Runs Rampant”, and it looks like it’s time to follow that up. The current Texas measles outbreak starting in January currently stands at 198 with 11% hospitalization rate, and an outbreak in New Mexico has recorded 30 cases. There have been a total of 222 cases of measles so far this year in 12 different jurisdictions, with a hospitalization rate of 11%, compared to 285 cases in 2024 with a 40% hospitalization rate. Texas and New Mexico have the only “outbreaks”, with sustained community transmission thus far in 2025–the other cases are mostly isolated, and related to travel or unknown exposure. While I haven’t seen much coverage in the US media, Canada is experiencing a similar measles outbreak (or far greater if normalized to a population which is only 12 % of the US) with 168 cases so far in Quebec and Ontario. The most recently reported Canadian data includes 61 new cases in one week, suggesting their epidemic is still growing quickly. In my note of two days ago I touched on some vaccine pointers, particularly that exposed or high risk for exposure infants can be vaccinated as early as 6 months, but need to receive a further two doses of vaccine after age 12 months. I’ve received some questions regarding adults and the need for boosters. If you had documented measles because you were born before the vaccine came into use, then you are considered to have life long immunity. If you were born before 1957, then you are generally considered to be immune—but if you don’t have a history of measles or actual vaccination records, and you are at high risk for exposure, such as international travel, healthcare settings, or outbreak exposure, then you should get a booster dose. There is no down side to getting a booster if you had measles and don’t know it, or have been vaccinated with two doses in the past and have no actual records to confirm that. To be effective the vaccine must be administered within 72 hours of exposure. Measles outbreaks around the world have ramped up in the post-Pandemic period. For some historical perspective, in the pre-vaccine era, it is estimated that world-wide 6 million children died every year from the disease. The following table shows the top ten countries and numbers of reported cases for the 5 month period of July 2024 to December 2024. Keep in mind of course that cases are vastly under counted in much of the world.
There is no specific treatment for measles; I could repeat that for emphasis, but I know many of you are already thinking, what about vitamin A which is recommended by not only RFK Jr., but the WHO, and the American Academy of Pediatrics (especially for children sick enough to be hospitalized). Vitamin A is an immune modulator supporting the normal functioning of the immune system, and it has been shown to have a beneficial therapeutic effect in third world settings, where vitamin A deficiency is high among children. No studies have shown a benefit in developed nations where vitamin A deficiency is rare, and no study has ever suggested a preventative role. It seems to me that the American Academy of Pediatrics (AAP) recommends it based solely on wanting to conform with the WHO recommendations, and not on any scientific evidence of benefit in a setting like the US. Unless your child is on a diet low in both retinol from dairy and animal sources, and low in carotene from plant sources, (basically malnourished on a highly restricted diet) the vitamin A that your church buddy, favorite influencer, or the previously mentioned august experts recommend will have negligible impact if your child contracts measles. On the other hand if you’re vaccinated you won’t need to be thinking about ineffective therapies.
If you are wondering why the price of eggs is so high again, consider the following statistics showing the numbers of poultry intentionally destroyed during the last 3 years in the US because of Avian Influenza infecting the flocks.

Since the 2022 outbreak began, more than 157 million birds have been affected (culled) by bird flu in the United States, including over 41 million chickens in December 2024 and January 2025 alone.
Government efforts to control the spread of infection have failed completely, and the toll will continue to rise. In my opinion we missed the opportunity to do an important experiment over the last 3 years—allowing the infection to rage through a large flock, and instead of killing every bird, use the presumably now immune survivors to reconstitute a new flock. We just might select for birds genetically much more resistant to the virus; the current approach counters the normal process of natural selection. Yes the infected flock would need very strict isolation, and rigorous PPE protection of people in contact with the birds—but such an experiment should be fairly easy. Long Island is the latest scene of wild bird die off, which has occurred around the country, with sightings of dead birds reported from multiple beaches.
Until now the highly pathogenic Avian Influenza H5N1 infecting poultry farms in the US has remained susceptible to olseltamivir (Tamiflu), and infected workers have generally been treated with the drug, and exposed household members given prophylaxis. A recently published report from Canada in Emerging Microbes and Infections details a strain of the virus with a mutation conferring high level resistance to olsetamivir. It has been thought, based on limited evidence, that this mutation would reduce the fitness of the virus—but these researchers report this new clade of H5N1 has spread rapidly and lethally through multiple Canadian poultry farms. This clade of the virus contains a reassortment of the neuraminidase gene between the typical Canadian clade of the virus and the prevalent American clade.
Neuraminidase reassortment and oseltamivir resistance in clade 2.3.4.4b A(H5N1) viruses circulating among Canadian poultry, 2024
https://doi.org/10.1080/22221751.2025.2469643
Despite evidence to suggest this substitution reduces viral fitness, viruses harboring this substitution spread rapidly across 8 farms in the 15 days following its initial detection," the researchers wrote. "As oseltamivir is the most widely used therapeutic and prophylactic against IAV [influenza A virus], the continued circulation of viruses harboring NA-H275Y may necessitate a re-evaluation of influenza treatment strategies in Canada." (NA-H275Y is the mutation)
H5N1’s acquisition of mutations allowing infection of mammals, and now high level resistance to oseltamivir, without compromising the virus’ fitness or pathogenicity in birds, are successive indicators of the “train wreck in slow motion”, we have been watching since 2022. While the clades of the virus infecting the dairy cows and poultry in North America have generally caused mild to moderate disease in the humans infected, the lethal case in Louisiana and near lethal case in Canada are a stark reminder that other, similar clades of this virus in Asia, have a very high human mortality rate. The last hurdle for this virus is gaining the ability to spread between humans as easily as it does in birds and a wide variety of mammals. That done and we may have a much bigger problems than $8 dollar eggs.

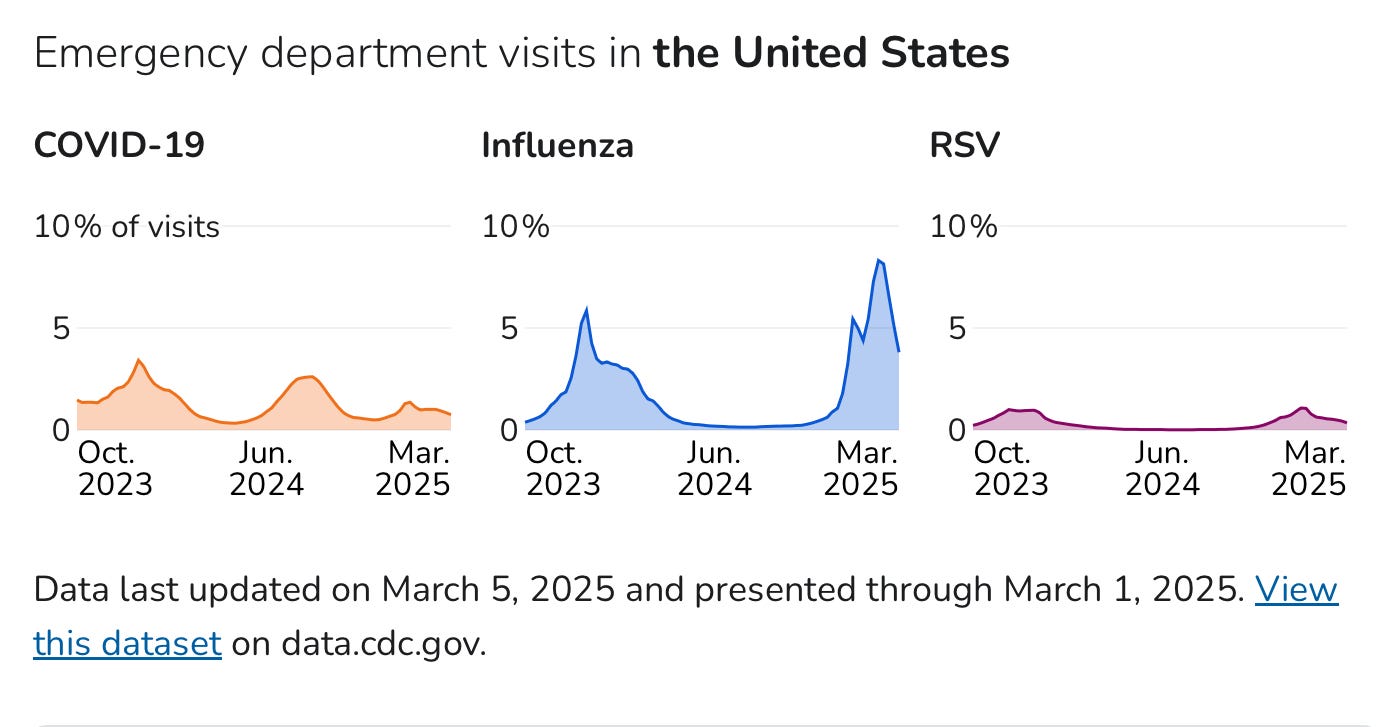
The most recent CDC data indicates that human Influenza activity is slowly abating with a second week of decreasing ER visits, and stable low COVID disease and RSV.
What goes around comes around, is frequently true in many aspects of life, not just pathogen ebb and flow. We could use a reset in civility and common sense in this country—but I don’t hold out much hope, and neither does Polymarket. Judging by questioning from both Republican and Democrat Senators it looks like Stanford Professor Jay Bhattacharya is a shoe in for NIH director. If you don’t recall, he was one of the authors of the Great Barrington declaration in the very early days of the Pandemic, which argued for keeping society largely open, no lockdowns, no school closures, and making attempts to protect the elderly and most vulnerable. They argued that this approach (during the time before vaccine was available, and no certainty when that would happen) was the most compassionate and least damaging to society as a whole, “to allow those at minimal risk to live their lives normally to build up immunity to the virus through natural infection, while better protecting those at highest risk”. He was pretty viciously attacked by other academics, and the heads of the NIH and NIAID as a “fringe epidemiologist”, with multiple scientists publicly questioning his qualification to have an opinion, his intellect, grip on reality, and worse. That view was quickly picked up by the media and projected as: There is a scientific CONSENSUS, and these lunatics are violating it. Bhattacharya and his co-authors were in part basing their argument on the understanding that many COVID infections were asymptomatic or incredibly mild, and that with a lack of systematic population level testing, we were vastly over-estimating it’s mortality rate. To prove that point he undertook a study in March 2020, published in the International Journal of Epidemiology 2/22/21, which was a seroprevalence study showing that infections in Santa Clara county were 50 times higher than identified cases, and 40 times higher in LA county. Currently it looks like many people have come to believe that he was right, or at least that he was entitled to have a very well informed opinion—since nobody had any lock on the truth, or solid evidence of what we should be doing in the face of this totally novel pathogen. Now it looks like he will become NIH Director, and many of the scientists who behaved in decidedly un-scientific, and frankly obnoxious, ways will come seeking grant money. My bet is Dr. Bhattacharya has a crisp memory for these events, but will exercise his authority in a completely professional, scientific data, and logic driven approach. One of the points he made during his confirmation hearing was fostering respect for dissenting scientific opinions. In this era of massive government spending retrenchment, we will see if Bhattacharya exercises good judgement in the allocation of now limited resources.
You just never know who will get spun up or down, or round and round on Fortuna’s wheel. I won’t give you a list here, you know dozens of the best known characters. The world would be greatly improved if we stopped absurdly vilifying and dehumanizing folks we disagree with. Decent behavior is unfortunately more often the result of fear of punishment than moral compass—that’s ok too. Dissenting views are always welcome, but their authors will be kept in a list for future reference. The like button guards against writer burnout and ennui.
Nice 'dance of death' graphic