

What Is On The Covid Holiday Menu This Year?

World events have taken many people’s minds off COVID, but the virus is completely undeterred by any human preoccupation, and continues to follow evolution’s bidding one mutation at a time. I thrive on optimism, but you would have to be unusually optimistic, and also dead wrong, to assume we are not in for another winter surge in SARS2-Cov19 disease. In the previous post I highlighted the rapid increase in a variant HV.1 which is slowly eclipsing EG.5 in the US. Both of these are in the XBB lineage, and there is good data to confirm that, either infection with a variant from this family, or the new monovalent booster will increase protection from severe disease for those at high risk. But there may be a fly in the oatmeal, a curveball to the corner, or a new kid on the block, which changes the game.
JN.1 is a recently described variant from the Pirola family (BA.2.86), and while only limited sequences of this mutant have been found in five countries so far, mathematic modeling is projecting a very significant growth advantage over the other leading variants in France. In early September I discussed BA.2.86 (Pirola), the variant with an exceptionally high number of Spike protein mutations, and opined that despite its impressive array of new changes it was merely a scariant, because of it’s very slow growth advantage. JN.1 is quite similar to its parent BA.2.86, but with a very important mutation L455S, giving it a significant advantage in evading our prior immunity. Are we due for a major SARS2 evolutionary shift away from the XBB family, which has dominated for well over a year and is the basis for the new vaccine, to a derivative of Pirola? Data this week from Yunloug Cao’s lab shows that JN.1 has impressive escape from prior immunity—the greatest we have seen so far. Perhaps this variant will turn out to be the uninvited holiday guest for this winter—or just the latest scariant—a short interval should give us the answer. The following data from Cao’s lab shows the impressive reduction in sensitivity to neutralizing antibody activity of JN.1 in the presence of serum from people with prior XBB breakthrough infections. The lower the horizontal bar, the lower the mean neutralizing activity—and remember this is a logarithmic scale so small visual changes are greater than they seem.

For a comprehensive analysis of the mutations present in JN.1, you could have a look at this article by William Haseltine PhD. in of all places Forbes! Don’t bother unless you are well versed in molecular virology—which I’m not. Haseltine stresses the large number of mutations separating JN.1 from the variant used for the new vaccine XBB.1.5 and from HV.1. He details how many of these mutations COULD make JN.1 more infectious and more pathogenic, but he fails to mention that JN.1 is extremely similar to Pirola BA.2.86, which had so many people’s panties in a bunch but turned out to be a fizzle. That seems like unnecessary fear mongering to me.
JN.1: The Odd Man Out Among Omicron Sublineages William Haseltine PhD. In Forbes, October 26
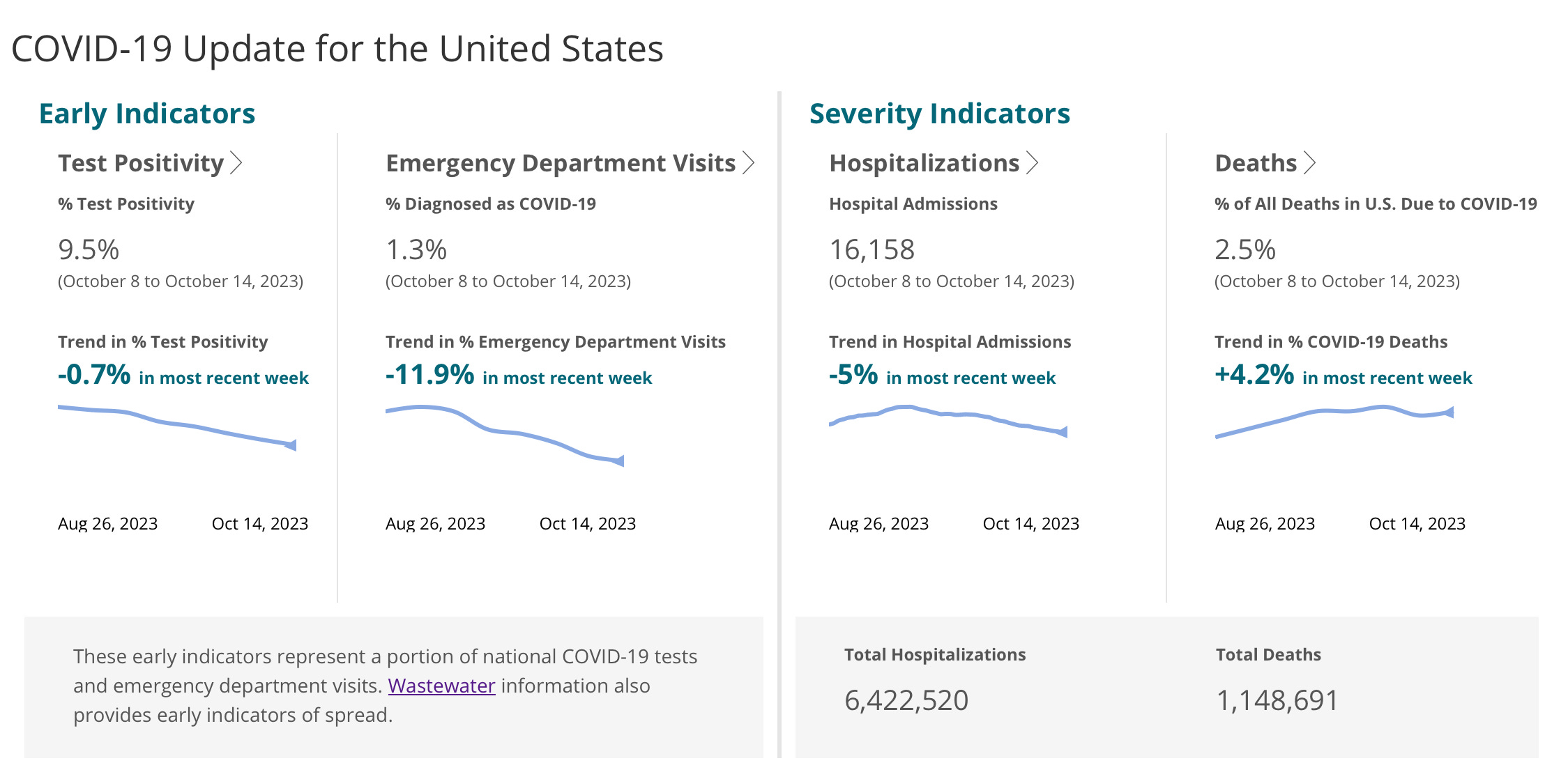
Let’s have a quick look at the current state of COVID in the US. Weekly new hospitalizations have decreased from a peak of 20,000 a few weeks ago to 16,000. Deaths have continued to rise, as indicated by the 4.2% increase over the last 2 week period, and COVID remains the leading infectious disease cause of death. In the last post I predicted deaths should start to fall by this week or next—let’s hope that happens.
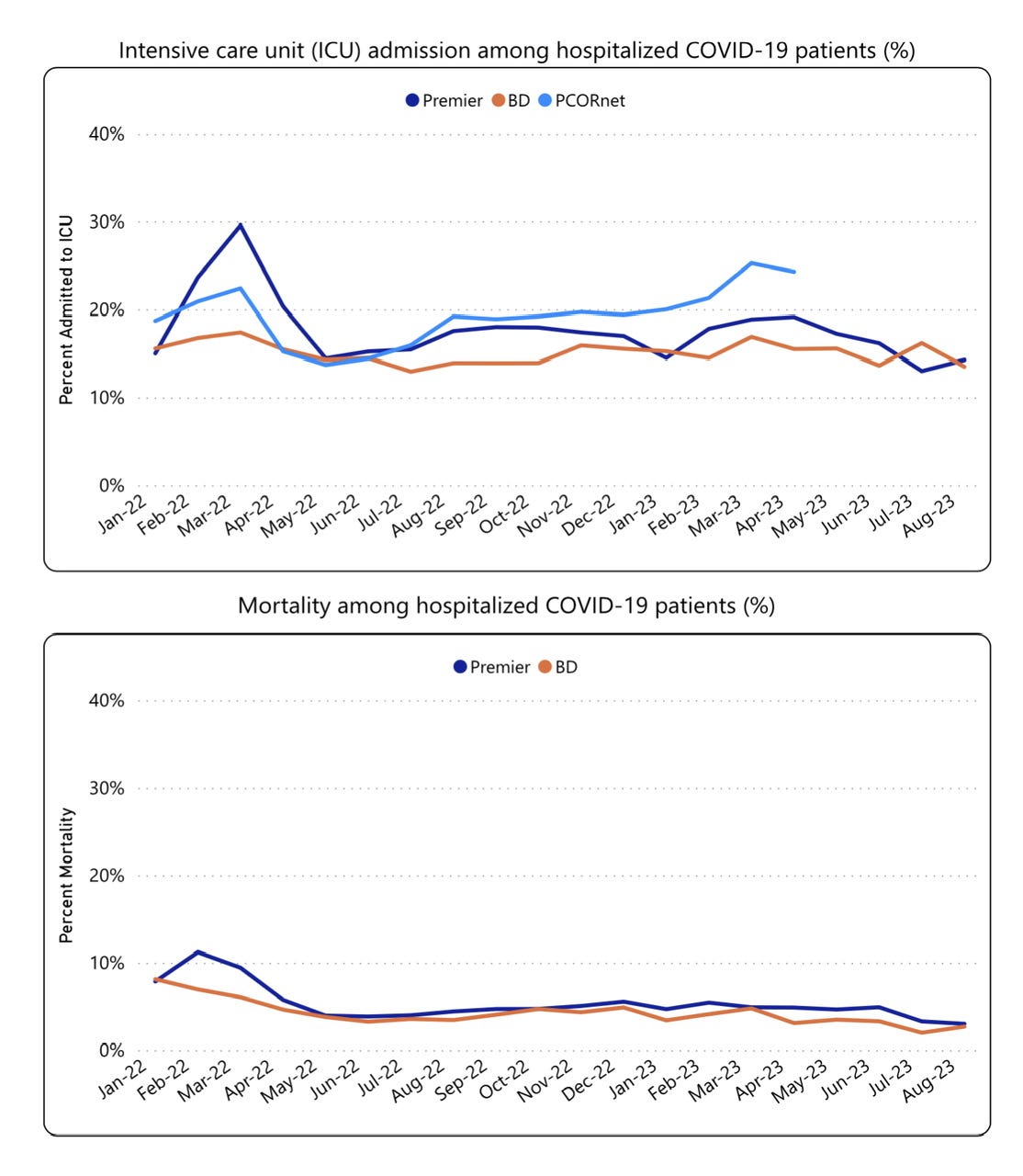
Here are two more CDC graphs which I find interesting. They demonstrate that if you are sick enough to make it into the hospital, then your chances of requiring intensive care, ventilation and death have not really changed over the last year and half. That is still the reality for the 16,000 people getting admitted to hospital every week, while the rest of us worry about other things. The different colored lines represent aggregate data from several large hospital networks across the country, one of which has stopped reporting this data. If you are very elderly or in compromised health, upping your immunity with a new dose of vaccine has been shown to greatly improve your odds of staying out of the hospital and off these charts if you get infected.
How about vaccine uptake? The people dying from COVID now are almost exclusively the one’s you can predict based on age and other co-morbidities, and the group truly in need of revaccination. The CDC reports that 3.6% of the population or 12 million folks got vaccinated since the new vaccine was released a month ago. Some voices are crying that the uptake is low because the funding (previously in the range of 100 million dollars) is no longer available for public education and “outreach”—but the uptake of vaccine in fact is tracking quite similarly to last year, when that money WAS available. It is possible that many people make up their minds about such things based on what they see and hear around them, from very personal experiences and observations; and perhaps take no notice of advertisements on buses, billboards and TV, or talks given by the director of the CDC, who is currently criss-crossing the country to drum up enthusiasm for the new vaccine. It is just possible all that money could have a more positive effect if it was expended on delivering direct health care for people who actually need and want it.
The last COVID related item today has some very important implications for your home testing, and how to logically adapt your behavior when you are sick. This study, published in Clinical Infectious Diseases, was undertaken because the authors theorized that increasing population immunity from vaccination and prior infection in the Omicron era would significantly alter the timing of peak viral loads. Sounds esoteric, but it’s not just counting how many angels can dance on the head of a pin. Earlier in the Pandemic we learned that SARS2 viral loads peaked either the day before or on the day that symptoms started, and then began to decline. A rapid antigen (home) test taken on the first day of illness had a very high chance of being positive. This study shows that now in the Omicron era viral loads are increasing until a peak on day 4-5 into symptoms. The practical implication is that viral loads may be low enough during the first few days of symptoms to give a false negative result, and you may go about your business unknowingly infecting others, or failing to start taking Paxlovid if you are at high risk for severe disease. We know that on average COVID today is less severe for most people, so why would the virus continue to increase in numbers for a longer period of days? It seems counter-intuitive until you consider that the onset of symptoms is really the result of our immune systems responding to the virus. Greater pre-existing immunity means the immune system turns on faster when viral loads are lower, and we experience symptoms sooner. Even if this phenomenon does complicate rapid antigen test interpretation; ultimately that earlier immune response is the reason that so many of us end up with a “cold” and not more severe disease. They also looked at Influenza and found viral loads in that disease peak very early on day 2. Here is the link and summary below.
The New Normal: Delayed Peak SARS-CoV-2 Viral Loads Relative to Symptom Onset and Implications for COVID-19 Testing Programs Clinical Infectious Diseases, ciad582, https://doi.org/10.1093/cid/ciad582
Results
Of 348 newly-diagnosed SARS-CoV-2 PCR-positive individuals (65.5% women, median 39.2y), 317/348 (91.1%) had a history of vaccination, natural infection, or both. By both Ct value and antigen concentration measurements, median viral loads rose from the day of symptom onset and peaked on the fourth/fifth day. Ag RDT sensitivity estimates were 30.0-60.0% on the first day, 59.2-74.8% on the third day, and 80.0-93.3% on the fourth day of symptoms. In 74 Influenza A PCR positive individuals (55.4% women; median age 35 yo. Median viral loads peaked on day 2.
For some good news on other vaccinations I would point you to a new study looking at the safety and efficacy of live viral vaccines in children with solid organ transplants. For many years it has been “received wisdom” in medicine that we shouldn’t give live viral vaccines (like Measles, mumps and rubella) to highly immune suppressed kids after organ transplantation (and other severely immunocompromised patients). The fear has been that the attenuated virus in the vaccine might cause the very disease it is designed to prevent. Yet this is the very population in greatest need of protection. This is the group at highest risk for severe disease or death from infection by these viruses—and that risk has been increasing as greater numbers of parents refuse to vaccinate their children, thus lowering the overall population immunity. The newly published paper looking at 260 immune compromised children vaccinated with MMR and VZV (chickenpox) is very reassuring in terms of safety, and surprisingly in terms of a very large majority having a protective antibody response similar to normal healthy children.
Feldman, A. G., et al. (2023). Safety and Immunogenicity of Live Viral Vaccines in a Multicenter Cohort of Pediatric Transplant Recipients. JAMA Network Open. doi.org/10.1001/jamanetworkopen.2023.37602.
That’s it for the science this week, the editorial page follows. Over the last 2 weeks we have witnessed scenes which frankly should have you wondering about the degree to which civilization is disintegrating. I have long maintained, without direct experimental evidence or randomized trial, that a good 10% of the human species would just as soon kill you as look at you—and that people spouting utopian ideas contrary to this are profoundly naive. The ease with which relatively normal people can be co-opted into cheering on savagery, and then pretending that they really didn’t mean to say or do that once there is a consequence is astonishing. Take away the consequences and the malignant element of the population feels no impediment to their actions. (Have a good hard look at the massive crime wave afflicting our major cities.). The US Senate has issued guidelines to its members and staff on how to lessen their chance of being a victim of car-jacking, and how to lessen their chances of being killed if it happens. Take away consequences, and another segment of the population will either turn a blind eye or gleefully participate enjoying the gratification of identifying with some group or movement. One way of looking at the “Woke” movement, which first took over our Universities, then Journalism and eventually corporate America, is that it attracted power by splitting people into smaller and smaller “victim”groups, and gave them the illusion of empowerment. (This was not the original inception of “Woke” which originated in African American circles as far back as the 1930’s, and referred to recognizing the genuine racism aimed at Blacks and particularly Black Women). Here I am referring to the “Woke” movement which originated in the environment of ultra-Leftwing Universities, and was originally pushed forward by the most privileged, elite, white faculty and students. Apparently once you identify as part of a group, which you are led to believe defines your entire being, then personal responsibility vanishes and many will do the group thing. Personally I don’t think the Germans on average were any worse than the population of other European countries—until they joined the Party (like Heinz the baker down the street, who was really a nice chap) then personal responsibility vanishes. It looks like this could be a watershed moment for Woke, as major cracks are appearing, and more and more people are noticing that most of the nonsense, which was counter to common sense, repugnant to any notion of fairness, or just down-right insane, can be made to go away. People don’t have to avert their eyes and pretend they don’t see it, believe that because it is pushed incessantly by the media it is now a permanent fixture of society; they don’t have to be afraid of it—they can turn around and say loudly that the Emperor Has No Clothes.
You don’t have to be a Democrat or a Republican to agree with me, in fact we would all probably be enormously better off if we didn’t identify with a particular political group. It would certainly lessen our collective cognitive dissonance. You can even disagree with me without being yelled at, called a name, or cancelled….that’s the fun part of not being Woke.
Thanks Jeff, excellent issue as usual. Can you tell us how viral groth advantage is determined for a particular variant?