What We Finally Learned About COVID Transmission
It’s the vaccinating season once again.

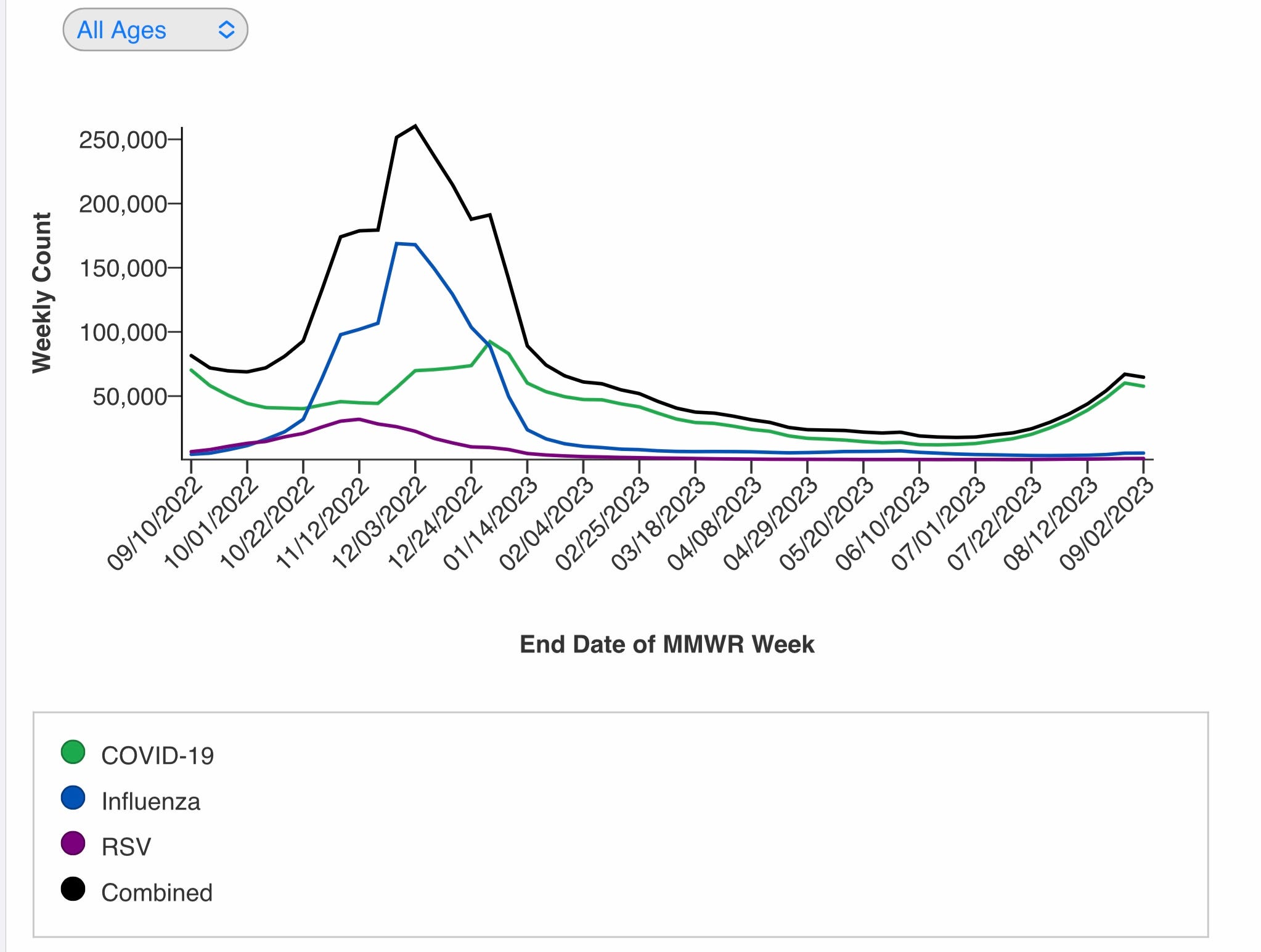
In my last post I had complained we were very close to the release of the new fall COVID boosters with no real data evaluating efficacy. That changed during the last week with release of data from Moderna and Pfizer on neutralizing antibody (NAB) responses to the XBB.1.5 monovalent boosters. Rather than go into detail, I think it can be fairly summed up as follows. The new boosters elicit a rise in NABS against XBB.1.5 variant in line with what we have seen with the earlier monovalent Wuhan booster and last fall’s bivalent BA.4/.5 booster. Of more interest is that the new vaccine formula shows a similar rise in NABS against other circulating XBB family variants, and also against EG.5 (Eris, now 21.5% of virus in the US). Moderna also presented data showing a good booster response against the FL.1.51 strain, which had appeared to be perhaps more immune evasive than Eris, and which is currently increasing. The latest scariant with the unusually high number of mutations, BA.2.86 (Pirola for those reading the tabloids) has turned out not to have the degree of immune evasion scientists predicted from its panoply of base substitutions. In addition, its slow rate of growth so far suggests it is less contagious than other current circulating XBB family viruses, and the new fall vaccines generate a good level of NAB response, even a bit higher than against the currently dominant XBB family. That is all very good news. The less good news, is that hospitalizations and deaths have continued to rise for 6 weeks now, and we are over 18,000 new hospitalizations in the last week. The rate of increase however has slowed in this last week, and if that holds steady for another week then I think this wave of disease is running out of steam and plateauing. An amusing story appeared in the NYT this past week about the “Flu” going around the US Open among spectators and competitors. Quite a bit of respiratory disease, which everyone is anxious to call the flu, but few were willing to test for and find it was in fact COVID. Folks who were previously adamant about their personal duty to protect others, now seem more concerned with their pricy tickets, and athletes not willing to be tested positive and thus lose an opportunity for a handsome payoff. In the words of Kurt Vonnegut, “And so it goes.” The following graph shows that the vast majority of the flu going around the Open is in fact COVID.

This week the CDC and the ACIP both gave the go ahead for distribution of the new XBB.1.5 boosters from Pfizer and Moderna, with the American Committee on Immunization practices voting 13 to 1 in favor of recommending the vaccines for use in all people over the age of 6 months. The two mRNA vaccines are both approved for use in individuals over the age of 12, and Moderna’s is authorized for children 6 mo. to 11 yo. under EU (emergency use authorization). Since the public health emergency was ended by President Biden in May I’m not sure how the FDA has the authority to approve the vaccines with emergency use authorization, rather than through the standard review and approval process. To me it appears contrary to the guidelines governing FDA actions—but these are still strange times.
You will be asked now to roll up your sleeve for the basket of vaccines for COVID, Influenza and RSV. What are the reasonable expectations of protection from the new COVID boosters? I think it’s a good bet that the experience this year will pretty closely follow last year’s booster results. CDC data just published in MMWR shows that protection from COVID disease severe enough to cause an ER visit or hospitalization was 65% in the first month after vaccination, but rapidly declined to 24% after 4 months. Protection from death was a bit more robust even out to 4 months. Currently the highest rates of hospitalization are occurring in the very elderly and in infants. Based on prior years experience, it is likely that the boosters will provide very limited protection from asymptomatic and mild to moderate infections. Infants below 6 months are protected to some degree by maternal antibody transfer, and of course their immature immune systems don’t respond to vaccines well. Folks at high risk of severe disease should certainly be considering the new booster as soon as possible, provided they have not had an episode of infection during the last several months. Although broadly indicated by the FDA and CDC, the RSV vaccine is something you should discuss with your physician; personally I don’t feel that the cost/risk/benefit ratio favors vaccination of healthy individuals simply because they are > 60 yo. The older you are, or with co-morbidities of pulmonary disease, CHF, or immune deficiency, the more likely you are to run into trouble with this virus, and significantly benefit from the vaccine.
Bivalent mRNA Vaccine Durability in Preventing Severe Disease https://www.medscape.com/viewarticle/992512
Next let’s review some very important recent data regarding the transmission of the SARS2-Cov19 virus. The mantra from the CDC and WHO early on in the Pandemic was that the virus was spread by large droplets spewed out when people cough, sneeze, talk or sing. Some transmission was thought to be from contaminated surfaces, but this was acknowledged to be a much smaller contributor. Both the CDC and WHO refused to admit that the virus was spread by microscopic aerosolized particles, which remain suspended in the air for long periods of time, even in the face of solid scientific evidence from the physical and engineering sciences. The direct results of the CDC’s failure on this issue was our population first being told, only doctors and nurses need to wear masks, just stay six feet apart please. Then we were told that we should (or must) wear masks, and that cloth masks and even surgical masks, which are completely inadequate to filter microscopic aerosolized particles, would work well. Now, using a novel technique, researchers from Northwestern University have published the results of experiments exactly quantifying the amount of virus exhaled into the air by infected people. Our prior understanding of viral dynamics was limited to measuring the amount of virus in the throat or nose, and a leap of faith that this would closely parallel infectivity. The results of these new experiments are illuminating, and have demonstrated that infected individuals excrete high concentrations of COVID into the air (up to 1,000 viral copies per minute) while simply breathing. Among their findings are: patients excrete virus at these high levels for the first 8 days symptoms before a rapid fall off, levels of virus were similar for the different major variants of concern, asymptomatic and minimally symptomatic people also exhale these high levels of virus, and that vaccinated people and unvaccinated excrete statistically similar levels of virus. What are the practical implications of these findings? First we need to rethink and experimentally study the way in which other respiratory viruses are spread, and question the “received wisdom” that they are conveyed mostly by large droplets. These experiments also show what many of us realized early on—that any mask short of a properly fitted N95 or KN95 was of minimal value. Next, it should put a further nail in the coffin in the idea of vaccine mandates at this time, and that the CDC guideline to isolate for 5 days is arbitrary and not supported by finding high level viral excretion out to day 8. Following is the link to this preprint.
Quantity of SARS-CoV-2 RNA copies exhaled per minute during natural breathing over the course of COVID-19 infection https://doi.org/10.1101/2023.09.06.23295138
The last item today concerns another virus which seems destined to be with us in perpetuity. The Chicago Department of Public Health has reported a cluster of mpox cases occurring at a time when generally only single cases were sporadically being identified. In a short interval of time they observed 13 cases of mpox. Most concerning is the fact that >70% of the affected individuals had been vaccinated with 2 doses of Jynneos vaccine, or the single recommended dose of the alternative ACAM2000 vaccine. This would suggest a fairly low vaccine efficiscy . The patients all belonged to the usual high risk group. As I pointed out when Jynneos vaccine was initially recommended, the vaccine had never been tested or approved for this disease. (See Monkey Business with the Pox Vaccine). The situation was further complicated by the decision to stretch the supply by administration of reduced doses intradermally instead of by the intra-muscular route. You might argue that something is better than nothing, but that is not generally the standard used to judge vaccines. The question of durability of the immune response is also completely unknown. Even more concerning is that communications aimed at the people at risk have stressed vaccination over behavior modification. This may easily lead to a false sense of vaccine security when the reality is that much more cautious behavior is still warranted.
This winter will test our accumulated immunity wall against COVID infection once again. It will also test how we utilize the growing body of scientific evidence to formulate rational decisions, both on a personal and societal level. Thanks for reading here. Please forward my work to your contacts who may be interested.
Thanks for making all the facts easier to understand! Hope all is well with you:)