

Why The COVID Crystal Ball Is Cloudy
Trust is hard to build and easy to shatter.

The FDA held its VRBPAC advisory committee on January 26 as a first step toward determining policy for COVID vaccinations going forward. About the only thing that’s clear so far is that the FDA will be moving to institutionalize once a year COVID boosters in the fall of each year, with a committee of experts to decide on the exact variant composition each July. Likely that will be a bivalent vaccine, at least for this coming year. If they settle on a once a year booster, the timing is certainly correct, as the pattern of maximal disease burden during an early winter peak has declared itself. Beyond that, it would be nice if they admitted they have no clear picture of what may happen next, of the timing or severity of a radically new variant, of the true value of bivalent boosters versus monovalent, and of the widely different boosting requirements of various demographics within the population. A standardized once a year vaccine for everyone at this point in time may be too much for many, and not enough for others at risk for severe disease. The low level of bivalent booster uptake (19% of eligible persons) is an issue we have already discussed. One has to wonder what proportion of the pricey new fall boosters will actually make it into arms, and whether the folks at the FDA have any concern whatsoever about such things.
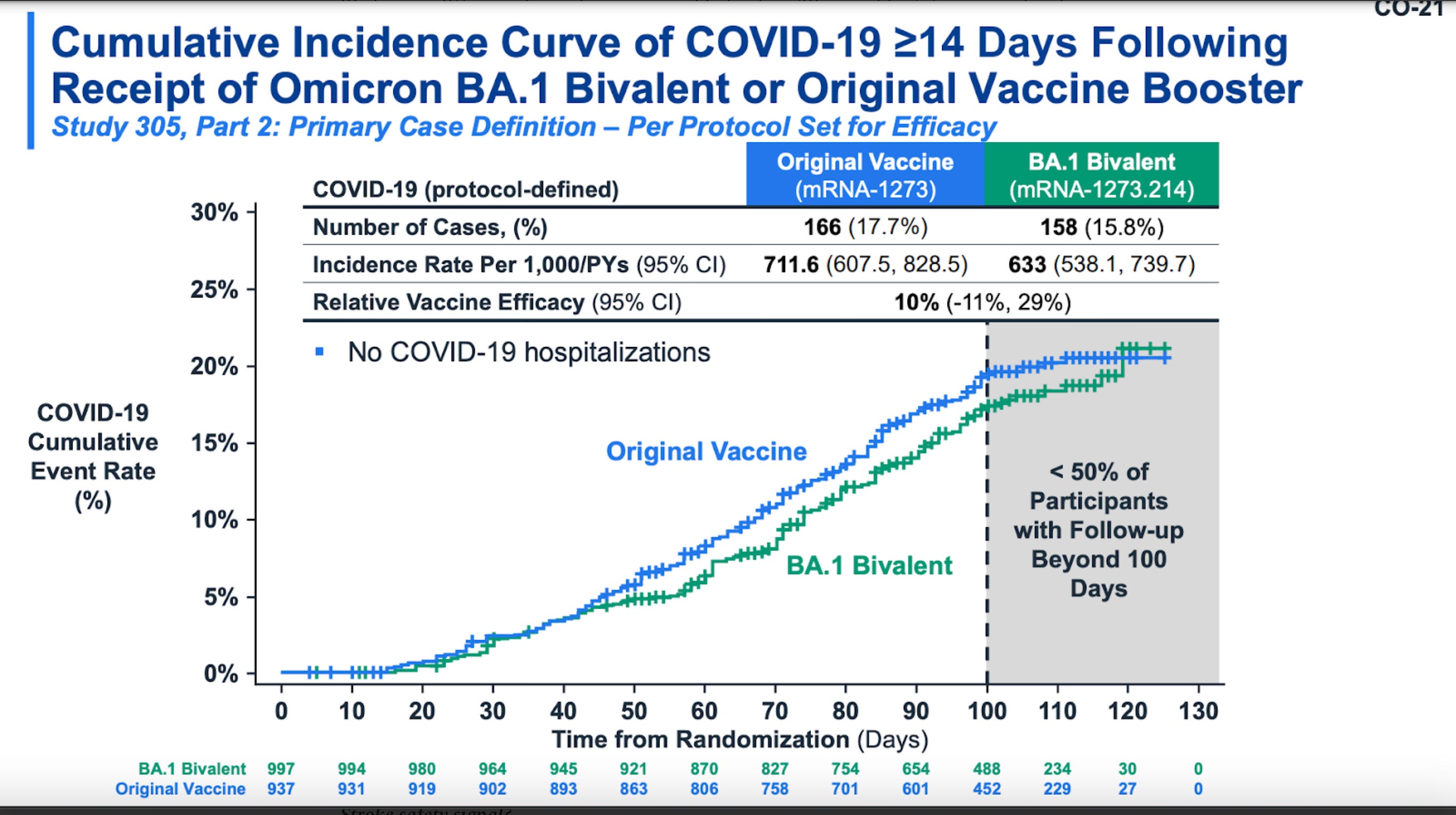
Moderna released new data from randomized controlled trial at the FDA meeting and published it as a preprint.
Lee IT … Das R. A Randomized Trial Comparing Omicron-Containing Boosters with the Original Covid-19 Vaccine mRNA-1273. medRxiv. 2023. https://doi.org/10.1101/2023.01.24.23284869
Some journalists (see Katelyn Jetelina’s: yourlocalepidemiologist.Substack.com) are banging the gong that this study “proves” the bivalent boosters work better than the old boosters. I won’t go into depth, but after reading the primary source I’m not impressed. The following graph from the study is a Kaplan-Meyer curve of the two booster regimens over three months. The numbers of cases of illness are low, the curves are identical for the first 45 days, then diverge to show a relative efficacy of +10% at 100 days for the bivalent. After 110 days the curves begin to converge again and it looks like any difference may be gone by 120 days. Maybe other studies will confirm this—maybe a short lived 10% increase in ability to prevent disease was worth billions in new vaccine acquisition.
Can we glean any useful information from the past behavior of the virus, or is the crystal ball still too cloudy? Below is a graph from Biobot lab showing the national average amount of SARS2-CoV in the waste water for each of the last 3 years. This is an accurate reflection of the amount of COVID virus circulating around the country, and as we know, is independent of whether people have access to, or an inclination to get tested. The years are superimposed, so seasonal patterns can be easily discerned. Beyond the remarkable synchronization of the winter peaks each year in early January, there doesn’t appear to be any other important seasonal pattern. For easy reference dark blue is year 1, light blue is year 2, and green is the last calendar year.
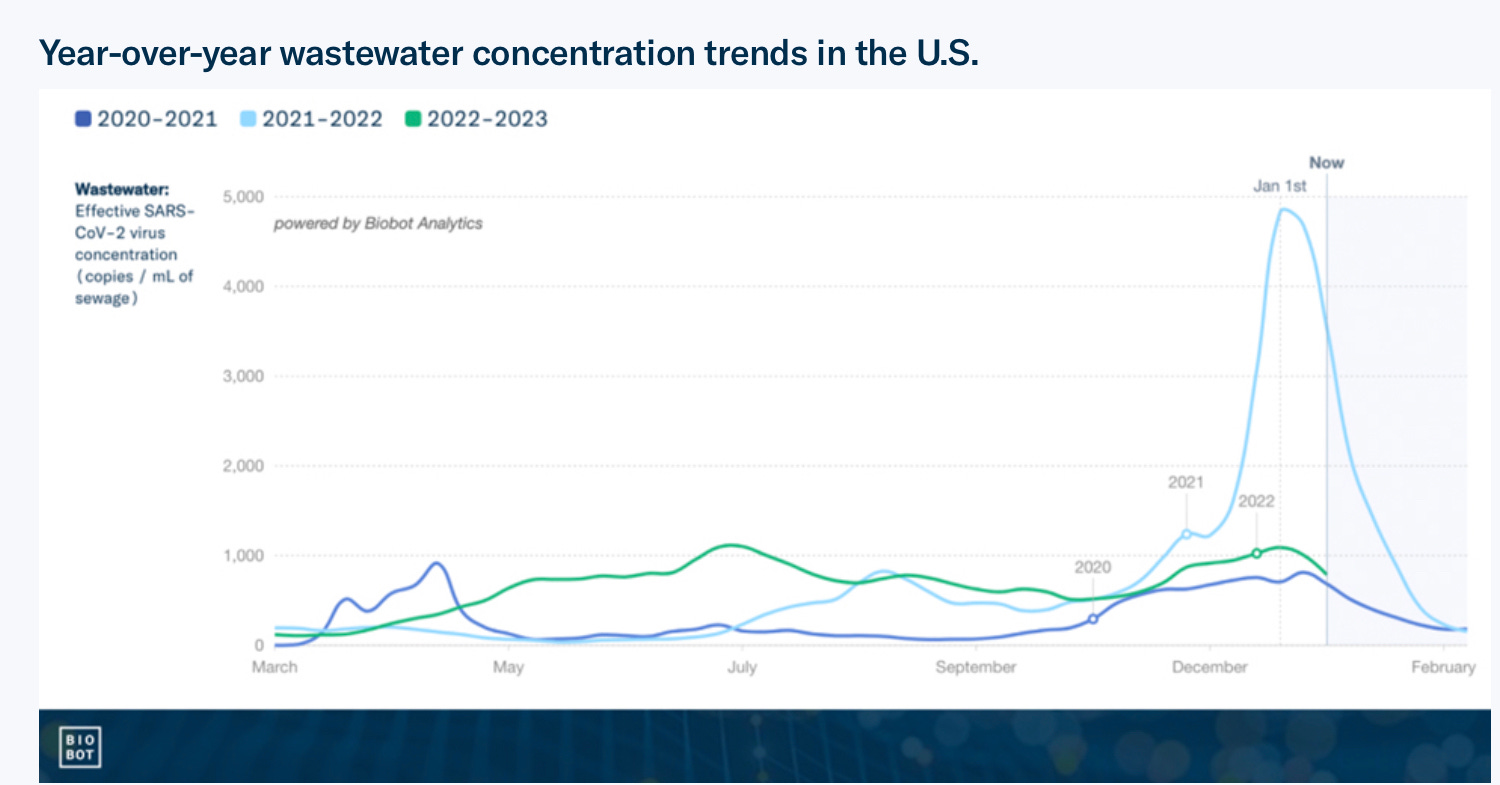
Just for a quick overview, the small dark blue peak at the left is the start of all this misery, the dark blue winter peak later that year is the arrival of the first significant variant Alpha. The light blue late summer peak is the Dirty Delta variant, and the light blue Mount Everest of course is last winter’s Omicron the Father. Now that we have reviewed the catechism of variants, what about last year’s green line gives you pause? In my estimate, the past year is remarkable because we had sustained viral infection across the population at a higher level, throughout the entire year (minus the winter peak of Omicron) than the previous 2 years. How can that be, considering we have all that built up vaccination and natural immunity? One possibility is the relaxation of all the social mitigation factors, leading to increased spread. That’s a possible explanation, and likely a contributor, but in reality a great deal of mitigation was already abandoned by the previous summer. The more likely explanation is the evolution of the current crop of variants, which are vastly more contagious than the original Wuhan virus, and are butting up against vaccine immunity that is far less effective than it was against the virus it was specifically designed to thwart. Natural immunity, like the vaccine, is short lived to begin with—and we are dealing with a virus that has entered an accelerated pace of evolution four times faster than Influenza. So the good news is that proportionally many fewer people are going to the hospital and dying (still over 500 deaths/ day). The bad news is that over the last year there have been more infections than ever before, and more new significant trackable variants than ever before. The good news is, high risk groups for serious disease have settled down to the very young and the old (less than 6mo. and over 65yo.) which makes targeting a segment of the population for intervention a bit easier, and insures the hospital system won’t be overrun. But the virus has been running on all cylinders throughout this year, and I see no reason to think that will end anytime soon. It certainly won’t be influenced by a once a year booster—despite such jabs giving some short lived increase in protection to the high risk group. Every viral replication is a chance for mutation and a shot at Greek Letter stardom, so; “It’s the Math stupid”.
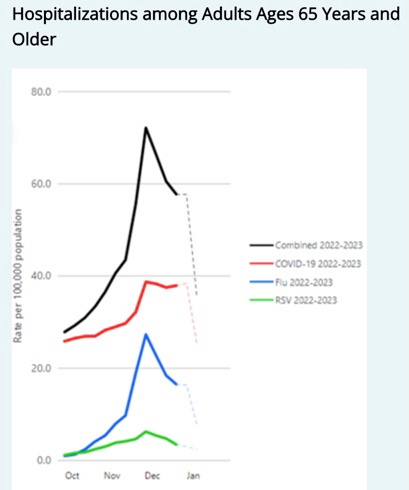
Influenza and RSV activity are both fading now, and we are starting to see a decline in new average COVID daily hospitalizations—down 13% from the previous week to 4200. XBB.1.5 is now estimated to be about 60% of the total virus in the US, and in many places, especially the east and west coasts, the worst of the winter surge is past. Some areas where XBB is not yet dominant may still see some small increase in hospitalizations over the next 2 weeks, but I think we are tracking right along with the previous winters and firmly on the downslope for now. The following is a graph through December 31 showing the relative contributions of COVID, Influenza and RSV to hospitalizations in people over 65. RSV is a minor player here, but obviously the story is quite different in the very young.
The last item for discussion today is the maelstrom surrounding Pfizer and the Project Veritas disclosure. The PV posting to YouTube shows a Pfizer executive secretly filmed, bragging about work Pfizer is doing to cause mutations to the COVID virus for study. My first reaction was to doubt this was really a Pfizer employee with the impressive title of Director of Research and Development- Strategic Operations and mRNA Scientific Planning. A bit of quick research on the web led to several lines of evidence suggesting that the figure in the video is indeed the Pfizer employee Jordan Tristan Walker. Only a giant corporation would be able come up with a title like that. This was further confirmed when Pfizer issued a statement directly addressing the issues raised by the video, and did not deny this was their employee. It boggles the imagination to think that this juvenile, feckless individual could possibly have anything to do with actual scientific research, and maybe he’s employed for other reasons, despite his title. My second reaction was, it’s almost immaterial whether Mr. Walker is telling the truth, his immature and casual buffoonery about a subject that involves the safety of mankind is catastrophic to trust in the pharmaceutical industry and virology research in general. My next impression was generated by Pfizer’s public statement issued two days later, and that was worse than what had come before. To my reading, the company statement assuring us that they don’t do Gain of Function Research, includes a clear description of activities they are pursuing “with collaborators” which are GOF research. It appears they are doing the same sort of experiments which some Numbskulls were doing at Ohio State. (I discussed this in the post, “Hubris in the Time of Catastrophe”) Then Pfizer continues, that if we still have concerns about GOF research, which they are not doing—rest assured that everything is being done in a Level3 Bio-lab. That’s about as reassuring as telling your Grandma she has nothing to worry about in the subway, as long as she doesn’t stand right next to the platform edge.
Now the devil is in the details, and there could be mitigating factors. Perhaps Pfizer did not clearly explain the nature of the experiments they are conducting. Perhaps Pfizer was too dense to deny this individual works for them, if indeed he does not. This is no time to bring out you communications Triple-A farm team. It sure looks to me like they are taking the highly contagious spike protein of new variants and combining it with the old original Wuhan Classic virus. Taking the more virulent and deadly, now extinct, Wuhan virus and giving it the keys to the kingdom with the latest and greatest evolutionary model spike. The final straw here was discovering that Youtube has banned the video, after 22 million views. Sure, you can still find it on the web if you look for it. In this era it seems the only thing big tech can’t keep from view is their censorship.
Thanks for sharing this read with everyone you can think of. I am trying to surpass the Project Veritas Pfizer views. Your comments in agreement or dissension are genuinely appreciated.
Question regarding the graph of wastewater trends; since you've been involved in the testing in your county you may have an idea of how frequent and/or the number of facilities/agencies had been doing this testing early on in the covid pandemic. I wonder what the graph means if the numbers of testing sites rose greatly during the 2+ year duration.