

Will COVID Tick or Treat for Halloween?
Deja Vu all over again, again…

One thing we have learned over the last 3 1/2 years is that COVID isn’t in the habit of telegraphing its plans anymore than Putin or Zelensky. There is a late summer surge of COVID happening around the world currently; it started in the far east, and is now significantly impacting the UK, where estimated monthly cases increased by 200,000 over the last three weeks of July. The National Health Service reports a 40% increase in hospitalizations (a 29% weekly increase in COVID specific diagnoses), but that is starting from a low level and is not stressing the system at this point. As mentioned in my last post, here in the US we are continuing to see an approximately 5-6 weeks long increase in diagnosed cases, with a current CDC reported 12% weekly increase in hospitalizations. The CDC doesn’t report COVID death statistics directly anymore, other than to indicate that they are 1% or less than all US deaths. Whether that is more or less than the weekend gang murders in Chicago and Baltimore is for you to figure out.
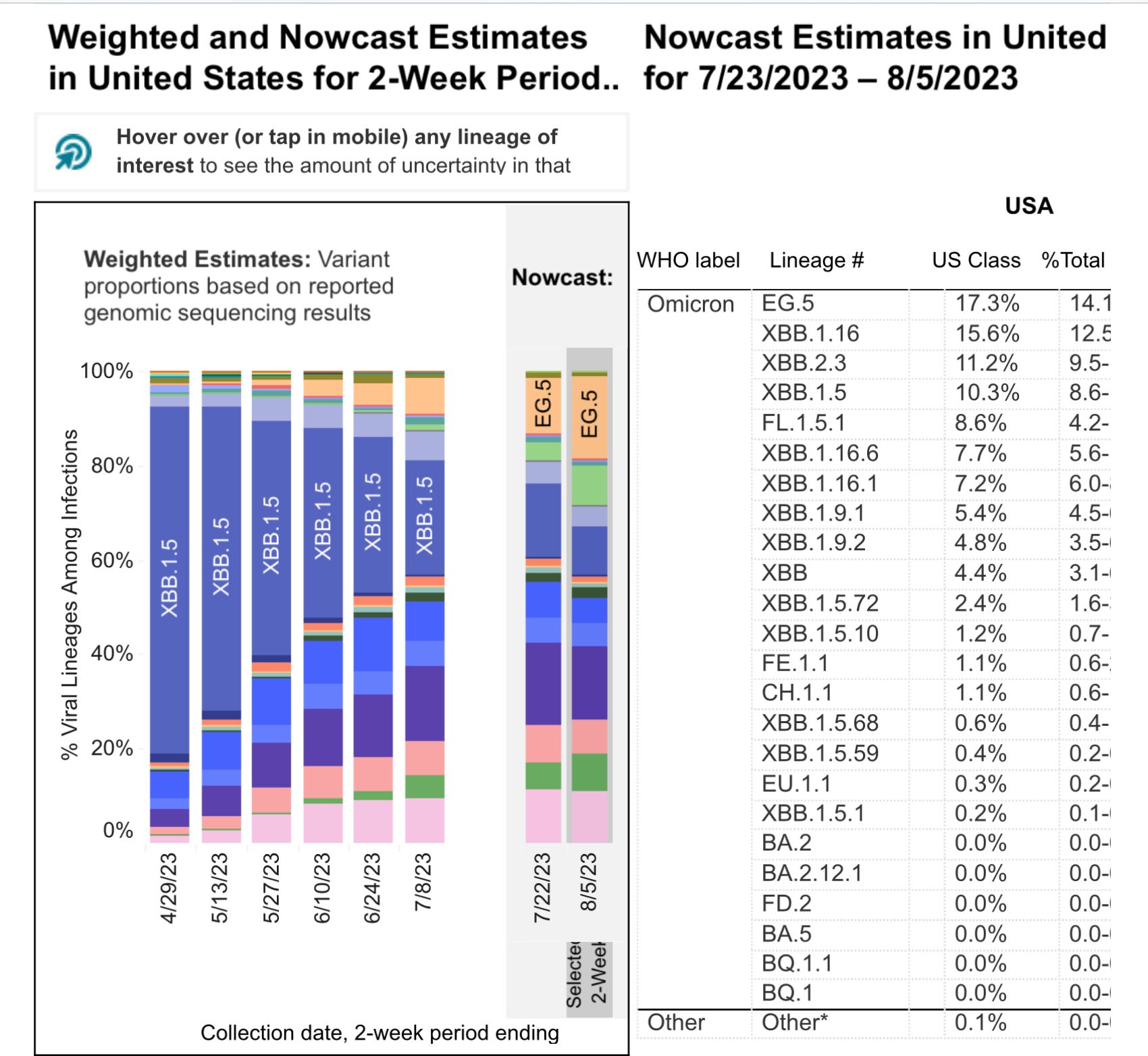
What is driving the current case increase has drawn speculation ranging from: the weather (it’s hot in the US, rainy in the UK—and it’s a safe bet to blame anything on climate change), to Barbenheimer bringing people into the theaters, to the appearance of the newest COVID variant to capture attention EG.5.1. This new variant, dubbed Eris by the media, has been on a roll rapidly increasing its relative proportion of total COVID sequences around the world. The following CDC Nowcast graphic shows EG.5.1 increasing at the expense of XBB.1.5, and currently projected at 17% of the US sequences. This increase in cases is almost certainly multifactorial, and the contribution of EG.5.1 is uncertain at this time.
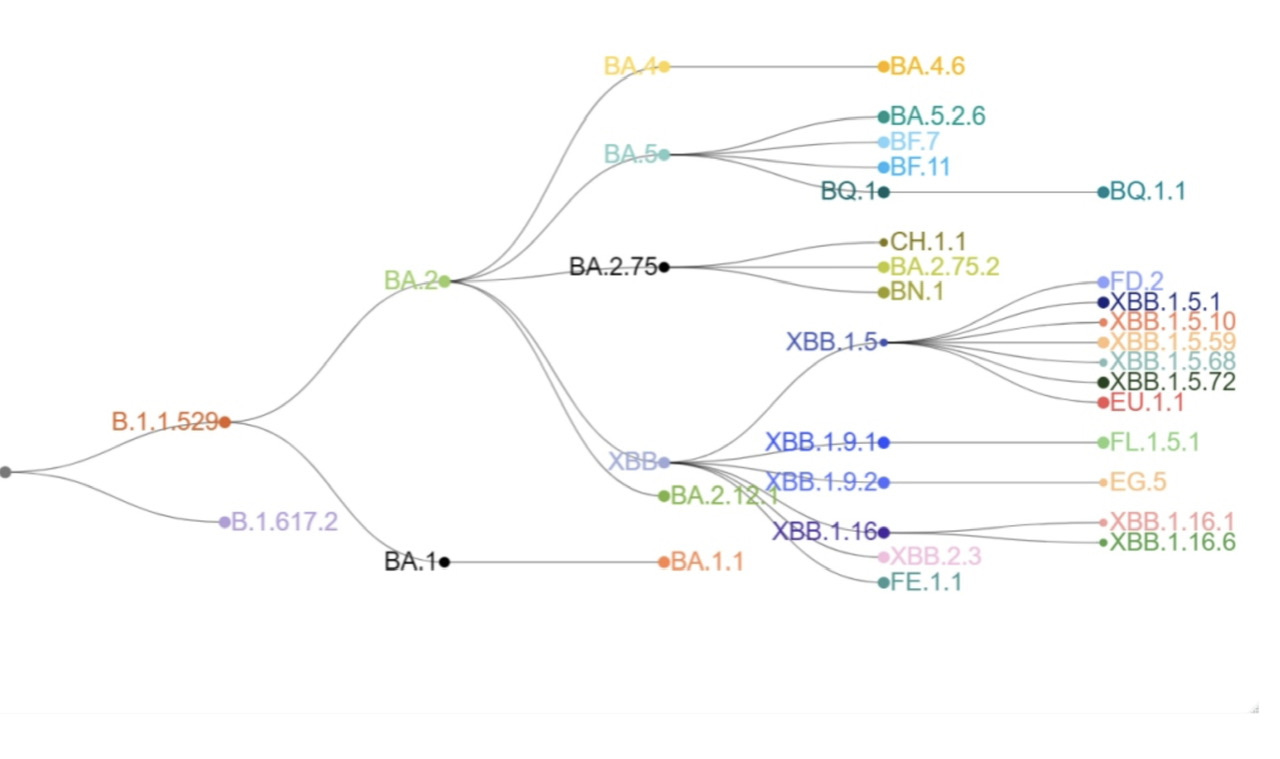
Don’t get lost in the weeds, but for those interested the following chart shows the evolutionary lineage of this Omicron the Father descendant.
What sets EG.5.1 apart from the crowd are two mutations in the Spike protein which are predicted to help the virus evade prior immunity. (Q52H and F456L) So what makes this deja vu all over again? You may recall that the bivalent booster rolled out for fall 2022 contained BA.5 (along with the extinct Wuhan virus). It didn’t take much imagination when the formulation of that booster was announced in June 2022 to predict that BA.5 would be history by the time the vaccine was manufactured and distributed. The result of course was that, last fall’s booster did offer a temporary increase in protection from severe disease (for those needing this), but extremely modest and very short term help in preventing infection. The same scenario is playing out again; by the time the vaccine is ready and needled up—XBB.1.5 will be history, and given the current trajectory, EG.5.1 or some other unknown assailant will be top dog. More on a potential unknown assailant further on. The prediction is once again obvious; we will see a temporary, maybe 4 month, increase in severe disease protection, and a short lived quite modest increase in protection from infection. The original timeline projection was for the fall booster to be available in late August to early September. In an interview with NPR last week Mandy Cohen, the new CDC director, suggested the shots may not be available until late October. That’s unfortunate for the segment of the population with genuine risk for severe COVID, most of whom are now quite distant from their last booster dose, with markedly waning immunity. I’ve been asked by several such folks, and others with special risk situations, if they should take another dose of the old bivalent booster. Given the high mutational distance between the old BA.5 and the current crop of XBB derivatives, plus the rapid rise of Eris EG.5.1, which is even further removed from BA.5, it makes no sense to get dosed with the old booster now. It is highly likely the new booster will be more effective. If you are at high risk, and the current wave of COVID continues on the ascent, then I recommend going back to the self protective mechanisms of social distancing, masking with N95’s, very limited short term exposure to indoor public spaces and assuming that basically anyone you interact with might be infectious, pending the availability of the new shots. For everyone else, relax it’s just the new normal—there has been a lot of that going around lately.
Looking a little further down the line at potential Holiday COVID is a variant discussed in a Tweet last week from Yunlong Cao, a researcher who has consistently contributed very useful experimental data throughout the Pandemic. (If this seems too weedy for you, skip to the quote below from Cao for the punchline). This variant has taken the novel approach of adjacent mutations in the RBD (receptor binding domain of the S protein). In addition to the F456L found in Eris, it has L455F. You will note that the amino acids L (leucine) and F (phenylalanine) are reversed, and this is being referred to as a Flip mutation. Individually, each of these mutations confer a degree of antibody escape, but at a cost to the virus in replicative fitness.
The L455F+F456L RBD [receptor-binding domain] mutation combo is a very smart move by the virus (it's actually an LF->FL shift)," Cao explained. "Note that both individual L455F or F456L actually lose ACE2 binding, but together, the LF->FL shift somehow strengthened ACE2 interaction while destroying most antibody binding."
Right now this variant with the Flip mutation in the RBD is a tiny 2% percent of world wide sequences, but it is rapidly taking over in a few locations like Brazil and Spain.
My guess is that EG.5.1 is not going to cause any dramatic surge in hospitalizations despite its antibody escape mutation. Below is the latest CDC graph of US COVID hospital admissions.
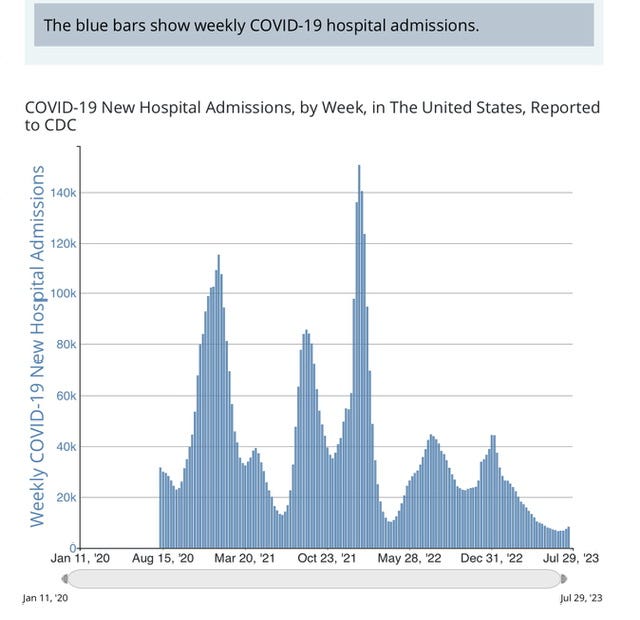
I’m basing that prediction on the following extremely rigorous mathematical modeling. The trough coming out of our lowest level inflection point around June 26 is U shaped and not V shaped—those U shaped ramp ups generally have lead to lower peak case numbers than the rapid V shaped take offs. For anyone interested in the details of my mathematical model, I have to tell you most of it has been redacted by the FBI. However, when you take a virus with substantial antibody escape and combine that with increased affinity for the human ACE2 receptor, there is the potential for significantly improved replicative fitness, and both increased transmissibility and severity. Let’s be watchful for COVID in Flip garb to visit Halloween or the winter holidays.
Two more issues on vaccinations. As you know the FDA recently approved two RSV vaccines for people over the age 60. The reduction in severe lower respiratory illness in high risk persons was impressive, and we reviewed the data in an earlier post. What is different about the current messaging from CDC regarding this vaccine is the emphasis on “shared decision making” between individual people and their physicians, rather than issuing a blanket recommendation that everyone over 60 get the shot. The reality is that a healthy 60 year old is at extremely low risk of very severe RSV disease. The older you are, with the presence of significant heart and lung disease or immune compromise, the risk goes up. There will be a cost consideration for many people as well. While we are discussing cost, let’s not forget that the era of free COVID vaccinations is over, and we are transitioning into the pay as you go model, which defines all aspects of life outside Washington DC. Add in the uncertainty of insurance reimbursement, the virtual disappearance of COVID from the major media, shuttering of many community vaccination sites, and the strong desire to, “Put this Pandemic stuff behind us”, and I suspect uptake of the new boosters will be lower than last year. That might be of little consequence to a majority of people, but a shame if it extends to the folks at high risk. Many people were planning on one trip to get both COVID and Flu vaccines. If the new COVID boosters are delayed as now suggested, the potential of two or three trips (counting RSV) isn’t likely to help turnout.
The final point today is about summer recreation. It’s that time of year when many people find their way to country fairs and rodeos. The CDC last week reported on two persons in Michigan who contracted a swine influenza after close contact with pigs at a fair. To be clear this is not the Swine Fever virus killings pigs around the world, which I discussed a few weeks ago. This is an influenza virus infecting pigs which is nearly identical to the human H1N1, and is sometimes passed from animal to human or vice versa. The subsequent illness is generally not severe for a normal healthy human; however, what is of concern, is that pigs may become simultaneously infected with both the current pandemic Avian Influenza and an H1N1 or similar virus which is highly contagious to pigs and humans. Reassortment of the viruses in the swine could lead to an Avian flu virus with human to human transmissibility. In our lifetimes we have encountered pandemics and epidemics with a variety of completely novel viruses: HIV, SARS1, Ebola, MERS, and SARS2-Cov19. It would be naive to think that we won’t see a highly significant event from a new twist on a virus which is present literally everywhere in the world. So enjoy the county fair, maybe even take in the pigs if they‘re your cup of tea—realistically the odds are firmly on China to be the source of any avian-pig-human viral scourge.

Thanks for your time and attention today. The Pandemic plus inflation have been hard financially, so the yearly subscription is increasing to the requirement that you buy me a drink if you encounter me in any South Sudan bar showing Seinfeld reruns in lieu of World Cup soccer. Please forward this to at least one person, swine or avian.